Playlist
Show Playlist
Hide Playlist
Case: 65-year-old Man with Cognitive Dysfunction

-
Slides Introduction to Dementing Diseases.pdf
-
Download Lecture Overview
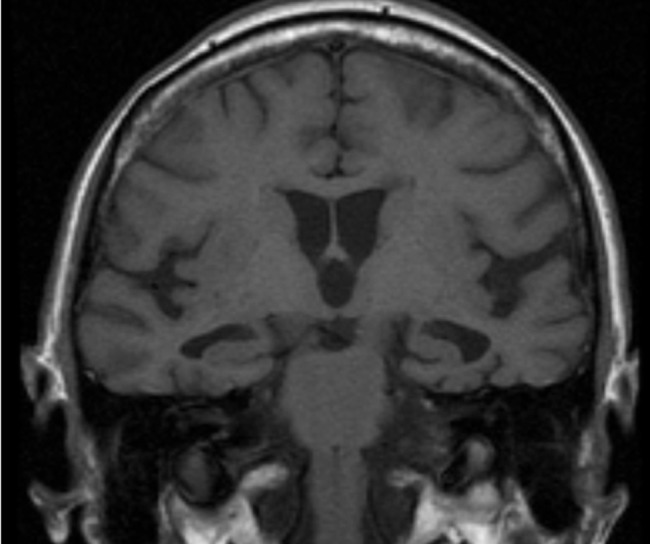
00:00 In this talk, we're going to review the dementias. Let's start with a case. This is a 68-year-old man with a history of hypertension, hyperlipidemia, and diabetes and prior brainstem stroke without residual deficits who presents with complaints of memory loss. The patient says that over the past year or so, he has noticed increased difficulty with remembering things. Initially, he would forget dates, appointments, names of acquaintances, and meetings. He is no longer working and retired about 6 months ago but denies that the memory complaints were the cause of his retirement. He manages his finances and drives and is able to complete other routine instrumental activities of daily living. He denies depression. He takes 2 blood pressure medications; a statin, metformin for his diabetes, and a daily aspirin 81 mg. 00:56 Examination is nonfocal. A MOCA, or Montreal Cognitive Assessment Test is performed and demonstrates a score of 24. So what are you thinking about with this case? Well, let's talk about some of the key features that I'd like for you to hone in on. 01:12 First is the symptom onset. This began a year ago and has slowly worsened over time. That's a chronic onset condition and we think about degenerative conditions and sometimes neoplasia as well as metabolic deficiencies and occasionally toxins. 01:28 The second is some of the key symptoms. This patient presents with cognitive dysfunction primarily in the memory domain. He has difficulty remembering dates and appointments, this sounds like an amnestic form of disease. The next is the impact on function. And while he does have cognitive complaints, they are not interfering with his activities of daily living, instrumental activities of daily living and in general his function. He is able to continue to do the things he needs to do. And in the last is his MOCA score, and we'll talk more about the MOCA which is a test for cognitive function and how we evaluate patients for mild cognitive impairment and dementia and his score is 24. So, what's the most likely diagnosis for this patient? Is this Alzheimer's dementia, frontotemporal dementia, Lewy body dementia, or mild cognitive impairment? Well, this doesn’t sound like Alzheimer's dementia. The patient presents with cognitive dysfunction, but it's not impacting daily function, which is an important criterion for diagnosing Alzheimer's dementia. This is not the presentation for frontotemporal dementia which presents with aphasia, speech dysfunction, behavioral changes, and semantic dementia, and that's not the prominent symptoms present in this case. This is not Lewy body dementia. Lewy body dementia is characterized by a combination of Parkinsonism and early cognitive dysfunction that often is subcortical with difficulty with executive function and speed of thought and verbal fluency. This is the typical presentation of a patient with mild cognitive impairment and specifically an amnestic form of mild cognitive impairment. The symptoms that are present are primarily memory, the MOCA supports MCI as opposed to frank Alzheimer's dementia, and there's non-impairment of the patient's activities of daily living.
About the Lecture
The lecture Case: 65-year-old Man with Cognitive Dysfunction by Roy Strowd, MD is from the course Introduction to Dementing Diseases.
Included Quiz Questions
Which of the following are included in the differential diagnosis for symptoms of chronic-onset cognitive impairment? (Choose all that apply.)
- Neurodegenerative disease
- Metabolic deficiencies
- Neoplasia
- Trauma
- Meningitis
What are the key differentiating symptoms of frontotemporal dementia?
- Aphasia, behavioral changes, semantic dementia
- Apraxia, hallucinations, chorea
- Agnosia, aphasia, ageusia
- Hyperorality, hypersexuality, amnesia
What are the key differentiating symptoms of Lewy body dementia?
- Parkinsonism, hallucinations, impairment in executive functioning
- Choreiform movements and progressive motor dysfunction
- Supranuclear palsy, amnesia, autonomic dysfunction
- Gait instability, urinary incontinence, behavioral disturbance
Author of lecture Case: 65-year-old Man with Cognitive Dysfunction

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
