Playlist
Show Playlist
Hide Playlist
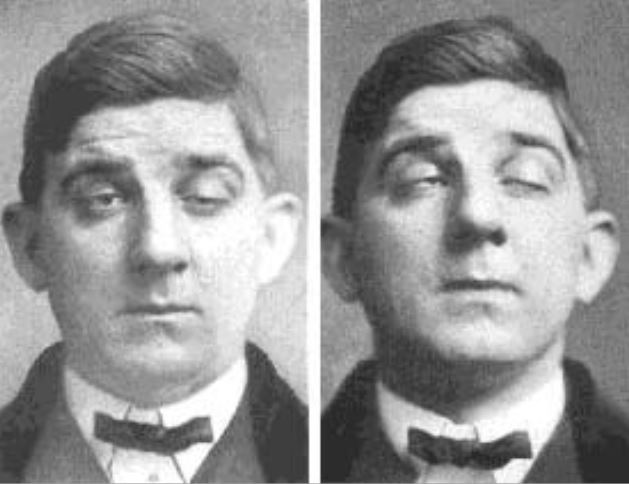
Case: 32-year-old Woman with Weakness and Sustained Upgaze

-
Slides Strowd Myasthenia Gravis.pdf
-
Download Lecture Overview
00:01 In this lecture, we're going to learn about Myasthenia Gravis. 00:04 This is one of the most common disorders that affects the neuromuscular junction, and a really critical disease to understand. 00:11 So let's start with a case. 00:12 A 32-year-old woman who presents with weakness and weakness is a common presenting symptom of peripheral nervous system disorders. 00:21 This 32-year-old woman presents for new evaluation of weakness. 00:25 She's noticed over the past two weeks that she's having trouble reading due to intermittent double vision, and has felt weaker when walking to the store. 00:34 She reports that her double vision worsens after she's been reading for 30 to 45 minutes, and that she's weaker when she's leaving the store compared to when she first starts shopping. 00:44 So some fatigability of her weakness and symptoms. 00:48 She's on no medications, has no major medical problems or prior surgeries. 00:52 And her examination reveals ptosis which worsens with sustained upgaze. 00:57 Again, fatigability. 00:59 Diplopia at extreme left gaze, and dysarthria that is more apparent at the end of your examination. 01:05 Again, fatigability. 01:07 She has no major other cranial nerve findings, and mild proximal weakness in both arms to four out of five. 01:14 Deep tendon reflexes are 2+, which is normal and symmetric. 01:18 Cerebellar testing is normal and there are no sensory findings. 01:22 So what's the diagnosis for this patient? Let's walk through those important three criteria for evaluating peripheral nervous system disorders. 01:30 Let's look at the distribution, sensory findings, and reflex exam. 01:34 The distribution here, she presents with proximal weakness. 01:38 But importantly, in addition to the generalized weakness is bulbar findings and bulbar symptoms. 01:45 She has ptosis, diplopia, and dysarthria. 01:48 And these are important findings to point towards a junctional disorder. 01:53 Sensory findings are absent since her exam is normal. 01:56 and this points away from a peripheral nerve etiology. 01:59 And the reflex exam is normal, which is supportive of a junctional disorder. 02:06 And importantly, we see some of those wildcard symptoms here fatigability, both in the patient's description and in our findings on examination. 02:15 And all of this points towards a junctional disorder. 02:18 So what was our workup? Well, nerve conduction study was performed with repetitive stimulation. 02:24 And we'll learn a little bit more about repetitive stimulation, which showed a decremental response with sustained muscle contraction and repeated muscle contraction. 02:32 there was less activation of the muscle. 02:36 Acetylcholine receptor antibody testing was performed, and was positive, for the presence of acetylcholine receptor antibodies. 02:44 So what's the diagnosis? Is this seropositive myasthenia gravis? Is this botulism? or Lambert-Eaton myasthenic syndrome? Well, this doesn't sound like Lambert-Eaton myasthenic syndrome. 02:55 There is a decremental response with repetitive stimulation. 02:59 And we can see that with any junctional disorder. 03:03 With Lambert-Eaton syndrome, we see an incremental response with rapid repetitive stimulation or sustained muscle contraction. 03:10 And we're not hearing about that here. 03:12 In addition, with Lambert-Eaton syndrome, we see a different type of antibody. 03:16 Antibodies to voltage-gated calcium channels for this presynaptic junctional condition. 03:22 So this doesn't sound like Lambert-Eaton syndrome. 03:26 What about botulism? Botulism is an infectious cause of a junctional disorder. 03:31 And we haven't heard of some type of exposure. 03:34 And the presence of acetylcholine receptor antibodies really points away from botulism and towards seropositive myasthenia gravis. 03:43 And this is a fairly classic presentation of a patient who has seropositive myasthenia gravis. 03:49 Proximal weakness with the presence of prominent bulbar findings, normal sensation and reflexes, fatigability and nerve conduction findings in serologic testing that strongly suggest and are indicative diagnostic of this type of myasthenia gravis.
About the Lecture
The lecture Case: 32-year-old Woman with Weakness and Sustained Upgaze by Roy Strowd, MD is from the course Disorders of the Neuromuscular Junctions.
Included Quiz Questions
In myasthenia gravis, nerve conduction studies with repetitive stimulation would most likely show which of the following?
- Decrement over time
- Improved muscle contraction
- Variable response
- Paralysis
- Hyperreflexia
In myasthenia gravis, antibody testing will show which of the following?
- Antibodies against acetylcholine receptors
- Antibodies against presynaptic calcium channels
- Antibodies that mimic the action of acetylcholine
- Antibodies against neurotransmitters vesicle docking proteins
- Antibodies against acetylcholinesterase
Author of lecture Case: 32-year-old Woman with Weakness and Sustained Upgaze

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
