Playlist
Show Playlist
Hide Playlist
Carpal Tunnel Syndrome: Diagnosis and Treatment

-
Slides Acute Inflammatory Demyelinating Polyneuropathy.pdf
-
Download Lecture Overview
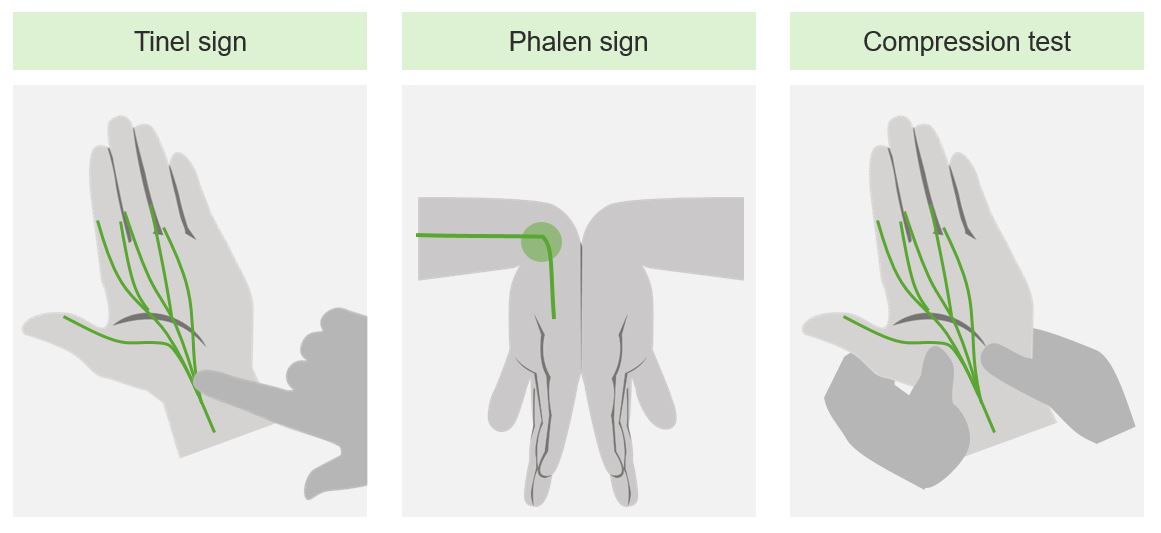
00:01 So, let's talk a little bit about mononeuropathies. 00:03 And I want you to remember three common mononeuropathies. 00:07 These are conditions that affect a single nerve. 00:10 Often at a compression site. 00:12 We think about median mononeuropathy, which is carpal tunnel syndrome. 00:16 Ulnar mononeuropathy which can occur at the elbow and is a sensitive compression site at the elbow, and fibular mononeuropathy in the leg. 00:25 Let's talk a little bit about carpal tunnel syndrome and use that to understand other focal compressive mononeuropathies. 00:32 In terms of signs and symptoms, patients typically present with pain, paraesthesia, weakness, and if not improved, or intervened upon ultimately atrophy. 00:41 as a result of compression of the single nerve. 00:44 The median nerve is susceptible to compression in the carpal tunnel, and you can see a cross section of the hand and wrist here. 00:52 The median nerve is sensitive to compression as a result of a number of things. 00:56 The first is all of the muscles that are beneath the median nerve and you can see that here. 01:00 And a tough fascial layer that extends over the wrist. 01:04 With repetitive injury or repetitive use, there's swelling of the muscles, there can result in swelling of the nerve. 01:11 And that window, that area that the nerve travels through is at risk for compression. 01:17 This results in focal dysfunction and problem in that nerve motor symptoms, sensory symptoms and ultimately atrophy. 01:25 There are a number of diagnostic tests that we can use to evaluate patients who present with numbness and weakness in the hands and evaluate for carpal tunnel syndrome. 01:34 And what we're doing is putting that median nerve in a potentially compressed situation to see whether that will reproduce the patient's symptoms of numbness and tingling extending down the median nerve distribution. 01:47 Here you can see Phalen sign, a demonstrated there and a positive Phalen sign will be reproduction of numbness and tingling, and paresthesias in a median nerve distribution. 01:57 And then Tinel's sign which is tapping over the median nerve as it travels through the carpal tunnel. 02:03 And again, a positive sign is reproducing the patient's symptoms numbness and tingling in a median nerve distribution. 02:11 To evaluate these patients, we can consider imaging although neuromuscular ultrasound would be probably favorable imaging as opposed to MRI or CT. 02:18 And nerve conduction study is the workhorse and gold standard of confirmatory testing when there are unclear clinical features. 02:27 Ultimately, the diagnosis of carpal tunnel can be made by clinical diagnosis. 02:34 Let's talk a little bit about median and ulnar neuropathies. 02:37 Those are the two nerves that travel out into the distal arm and are susceptible to compression. 02:43 Ulnar neuropathy may present with an ulnar claw. 02:46 The nerve involved is the ulnar nerve and it can be at the wrist. 02:50 We can also see ulnar nerve compression more commonly at the elbow. 02:53 The typical presentation is this appears in long standing cases of nerve damage. 03:00 The digits that are affected are the fourth and fifth digits. 03:03 We see muscles that can be paralyzed, and that's isolated to the medial to lumbricals. 03:08 And it tends to be that movements that are involved is unopposed extension of the MCP joints, and an unopposed flexion of the interphalangeal joints. 03:18 This is different than what we see with median nerve pathology, which is the hand of benediction. 03:23 Here lesions of the median nerve can occur at the elbow or wrist. 03:27 This appears when the patient attempts to make a fist. 03:30 The patient attempts to make a fist, and the fourth and fifth digit work but we don't see flexion and function of the first three digits. 03:38 This affects the lateral half of the flexor digitorum profundus and the lateral to lumbricals. 03:44 And there's inability to perform flexion at the MCP and IP joints of the three fingers. 03:50 And here's two schematics of the claw hand and hand of an addiction. 03:54 Seeing the claw hand should point towards the concern of ulnar nerve pathology, the inability to flex the fourth and fifth digit. 04:02 Whereas hand had been addiction should point towards problems with the median nerve. 04:05 And again, that's inability to flex the first three digits. 04:11 Let's talk a little bit more about how we treat patients with carpal tunnel syndrome. 04:14 Well, there are a number of steps we can go through to evaluate and manage these patients. 04:18 One of the first questions we have is, is the patient pregnant? Carpal Tunnel Syndrome is common more common in pregnancy. 04:24 It's one of the most common focal compressive neuropathies during pregnancy as a result of fluid shifts. 04:30 If the patient is pregnant, we wouldn't consider surgery and conservative measures would be pursued. 04:35 If the patient is not pregnant, we want to understand the severity of symptoms and we'll use our clinical exam and potentially electrodiagnostic testing. 04:42 If symptoms are mild, nonsurgical measures such as splinting, or corticosteroid injection can be considered. 04:48 For patients with moderate to severe symptoms, many of these patients would be referred for nerve conduction study and EMG (electrodiagnostic testing). 04:58 When electrodiagnostic testing is done, if there's evidence of axonal loss that indicates that already that nerve is de-innervated and there may be limited benefit with surgical decompression, and non-surgical measures, splinting corticosteroid injections are pursued. 05:13 But for patients without those end organ damage, axonal loss and denervation, surgical decompression to release the median nerve may be considered.
About the Lecture
The lecture Carpal Tunnel Syndrome: Diagnosis and Treatment by Roy Strowd, MD is from the course Acute Inflammatory Demyelinating Polyneuropathy (AIDP).
Included Quiz Questions
Which of the following nerves is correctly paired with its compression site?
- Ulnar nerve - medial aspect of the elbow
- Median nerve - lateral aspect of the leg
- Fibular nerve - carpal tunnel
- Fibular nerve - medial aspect of the leg
- Median nerve - lateral aspect of the elbow
Which of the following findings is most likely to be seen in ulnar nerve neuropathy at the wrist?
- Claw hand
- Benediction hand
- Phalen sign
- Tinel sign
- Rovsing sign
Surgical decompression of the median nerve is contraindicated in which of the following patients?
- A 29-year-old pregnant woman
- A 45-year-old man with well-controlled diabetes
- A healthy 35-year-old woman
- A 55-year-old woman with hypertension
- An obese 60-year-old man
Author of lecture Carpal Tunnel Syndrome: Diagnosis and Treatment

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
