Playlist
Show Playlist
Hide Playlist
Carotid Stenosis: Management

-
Slides CarotidStenosis Surgery V2.pdf
-
Download Lecture Overview
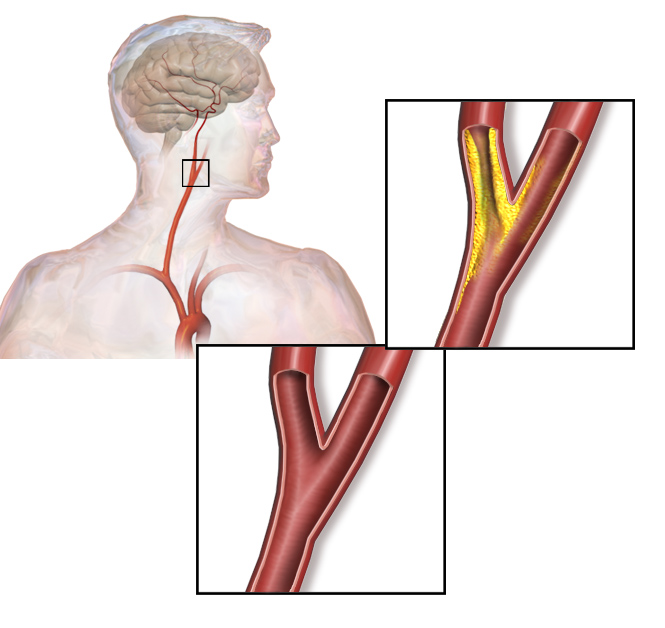
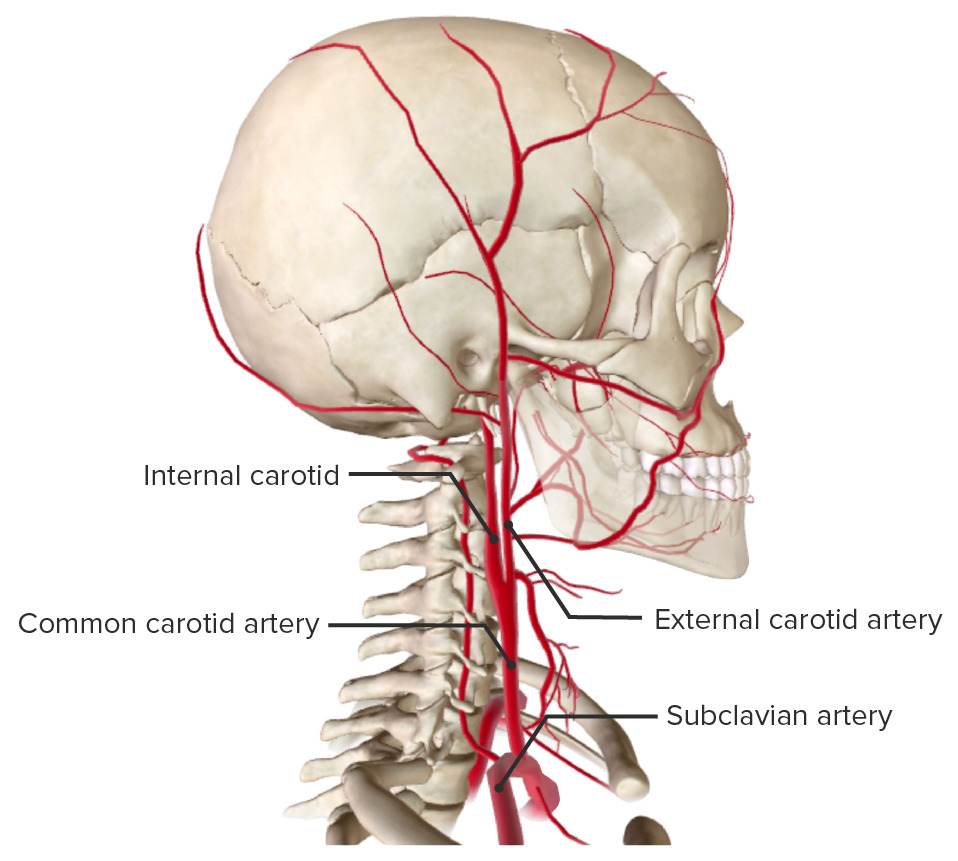
00:01 Now, that you've diagnosed carotid stenosis how do we treat these patients? Remember most patients with carotid stenosis particularly when they're symptomatic will require surgery. 00:13 We'll go over the surgical indication shortly. 00:16 Medical management include both lifestyle changes and pharmacologic risk reduction. 00:22 First antiplatelet therapy, whether that's aspirin or plavix. 00:28 Next, statins, as you know cholesterol lowering medications in the statin group have particularly -- are particularly useful for plaque stability. 00:39 Remember we use that in some patients with myocardial infarction all the time and reduce patients high blood pressure, specifically beta blockers. 00:50 What about lifestyle changes? Often times much easier recommended than actually achieved by our patients but if were you I would recommend the patient stops smoking, lose weight and decrease your alcohol consumption. 01:05 Unfortunately, these are at best preventative measures. 01:08 Here are the indication for surgery. 01:12 Our decision tree for offering patient with carotid stenosis surgery is largely dependent on whether or not the patient has symptoms. 01:19 Let's discuss symptomatic patients first. 01:23 In multiple perspective large trials, symptomatic patients with greater than 50% stenosis has diagnosed by imaging modality of choice are usually recommended to have surgery. 01:34 Of course, patients have to have greater than five years of life expectancy. 01:39 This is a particularly important because there are risk associated with this surgery, specifically stroke risk. 01:46 As a surgeon before offering the surgery to your patients, you must know your own complication rates. 01:53 The benefit have to outweigh the risks. 01:56 Next, let's talk about patients who are asymptomatic at the time. 02:00 Patients who have asymptomatic meaning no TIAs, no amaurosis fugax, who have high grade stenosis as defined by greater than 80% are usually offered surgery. 02:12 Additionally, if a patient has had a previous stroke, myocardial infraction and you suspect a chance of death for the surgery is less than 3% then if their carotid stenosis is greater than 70% they should also be offered surgery. 02:28 Lastly remember, annual surveillance from those not undergoing surgery is important just because the patient is not a candidate now doesn’t mean that their disease may not propagate. 02:38 If your patient is appropriate and meets indication for surgery, we offer carotid endarterectomy. 02:45 Here you see surgeon’s busy working at exposure of the neck. 02:50 Incisions typically made over the sternocleidomastoid muscle running just along your neck. 02:55 After the exposures achieved, this is what we see. 03:00 They particularly close the tension to the left side of your screen. 03:04 Blue vessel loops encircle the common carotid, external carotid and internal carotid arteries. 03:11 Shortly the surgeon will be expose in the carotid arteries, removing the plaque and widening the channel by doing what's called an angioplasty. 03:20 They'll place a large piece of graft covering all bifurcation allowing smoother flow. 03:26 Here's the depiction of what actually happens, the yellow plaque is identified, remove from the wall of the vessel. 03:35 It remained it at loss bits or tied down so there's no embolic phenomena and subsequently the hole that was made is closed. 03:43 As I previously described the vast majority of surgeons would actually place an angioplasty or a graft in this region so that the repair itself does not become stenotic. 03:55 Carotid stenting is another available option as well. 03:58 While trials have shown that has similar long term outcomes as an endarterectomy it does carry a higher periprocedural risk for the patient. 04:07 For these reasons, it is generally reserved for patients with a very high surgical risk as the shorter procedural time and less invasive nature of stenting may offer a net benefit to the patient. 04:19 Thank you very much for joining me on this discussion of carotid stenosis.
About the Lecture
The lecture Carotid Stenosis: Management by Kevin Pei, MD is from the course Special Surgery.
Included Quiz Questions
Which of the following criteria is NOT an indication for surgical treatment of carotid stenosis?
- 40% stenosis without symptoms
- 80% stenosis without symptoms
- 90% stenosis with symptoms
- 70% stenosis without symptoms
- 50% stenosis with symptoms
Pharmacological and lifestyle management for carotid stenosis includes all of the following EXCEPT?
- Lifestyle changes are not recommended
- Antihypertensives
- Antiplatelet therapy
- Weight loss
- Smoking cessation
Author of lecture Carotid Stenosis: Management

Kevin Pei, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
