Playlist
Show Playlist
Hide Playlist
Cardiac Case: 62-year-old Woman with Fever and Epigastric Discomfort


-
Cardiac Case 62-year-old Woman with Fever and Epigastric Discomfort.pdf
-
Reference List Cardiology.pdf
-
Download Lecture Overview
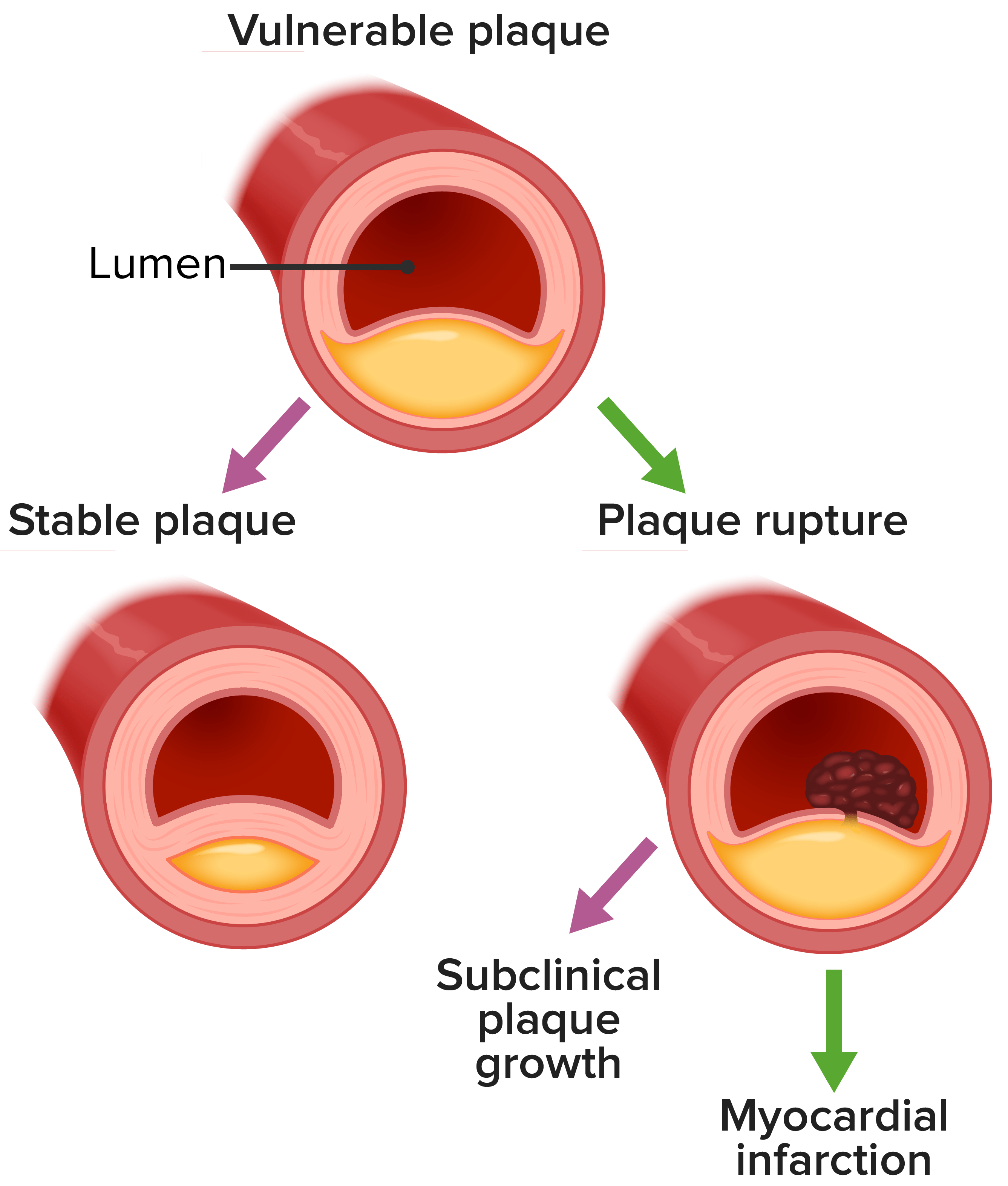
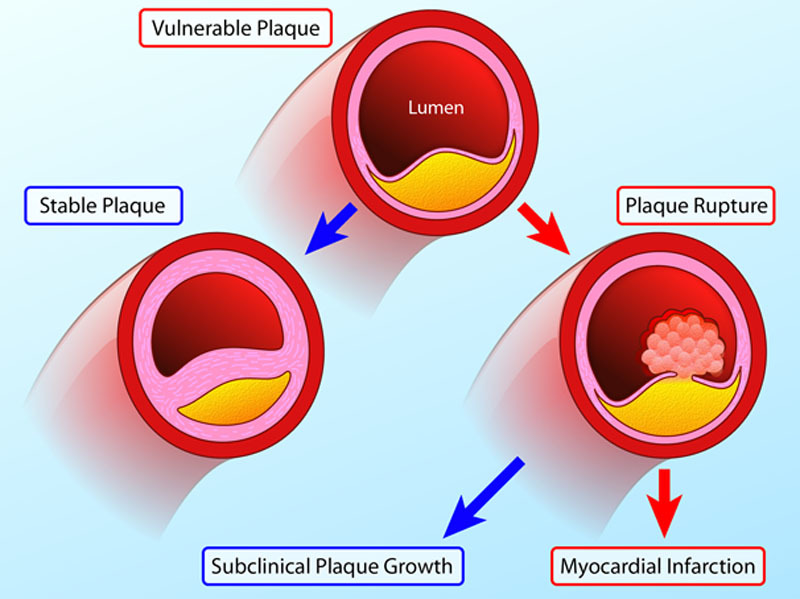
00:00 So this 62-year-old woman presents in the emergency room with a fever and this discomfort in her upper abdomen for two days. 00:09 She took some antacids thinking it was indigestion but didn’t help. 00:14 On physical exam her blood pressure is low 80/55, her heart rate is reasonable at 88 and she has an elevated temperature at 39.5 cm or 103.1 Fahrenheit. 00:28 Her jugular venous pulse is flat so there’s not right atrial elevated pressure, she has clear lungs so we’re not seeing any sign of heart failure. 00:37 She has an S4 but again as I said before that just means her left ventricle is a little bit stiff and that could be due to aging or a whole variety of cardiac conditions. 00:48 She has some tenderness and guarding in the right upper quadrant so when you feel here - oh, she says, that hurts when we press just under the right rib and we’re going to show you ECG and some lab values. 01:03 By the way, what’s going on here? There’s a fever that’s suggests an infection, there’s no signs of left ventricular failure and so but she has some signs that there’s something going on in her abdomen particularly on the right upper quadrant here’s her electrocardiogram. 01:23 Look at it and think about it for a moment. 01:32 So if you looked at it you would note that there’s ST segment depression in leads V2 through V6 squared off ST segment depression implying myocardial ischemia. 01:45 Notice for comparison that normal ST segment in the little strip below and that marked clear ST segment depression so this implies that there’s myocardial ischemia going on. 01:59 Well, of course with that she’s taken to the cath lab and there’s a 100% occlusion of her right coronary artery which is opened with a stent but the fever is something different, you don’t have a high fever with a myocardial infarct and you don’t have right upper quadrant discomfort, so some blood cultures are sent and the blood culture shows a little bit of elevated troponin that suggests myocardial ischemia and an injury to the heart but we already know that there was ischemia from a blocked coronary artery which we’ve opened up now, so what else is going on? Well, we do an echocardiogram and that shows that there’s lack of movement inferiorly so presumably this lady had had a myocardial infarct at some point possibly its relatively recent cuz the troponin’s elevated, her left ventricular ejection fraction is 40% so it’s reduced, normal - the lower limit in normal is 50% but we’re still worrying about her abdominal discomfort and her fever that doesn’t go with the myocardial infarct. 03:03 Well, we get an ultrasound, we had an echo ultrasound of her heart, now we’re getting an echo ultrasound of her abdomen, there’s stones in the gallbladder. 03:13 She has a dilated common bile duct which is a sign of a stone in the bile duct and sure enough she has an impacted stone in the bile duct and that’s led to an acute infection of the gallbladder, acute cholecystitis at the same time she had her heart attack, so she has two diagnoses - an acute non-ST elevation MI and acute cholecystitis. 03:40 Now, this has been discussed much in the literature - is it possible that the acute cholecystitis precipitated enough inflammation to cause the clot to form in the coronary arteries or did the myocardial infarction start first and somehow result in heightened activity in the abdomen and in the bile system that lead to the acute cholecystitis where there were already stones? We don’t know here which is the chicken and which is the egg, but we know the lady has two diseases. 04:13 So the diagnostic test that are subsequent, we checked her chest x-ray, make sure she’s not in heart failure. 04:19 We do a blood panel to assess kidney and liver function because we’re thinking about possible surgical intervention on her gallbladder. 04:28 We do a CBC which is a hematocrit to make sure she's not anemic and we looked at the white blood cell count. 04:35 In this case the white blood cell would be elevated because of the infection. 04:40 She’s already had her right coronary artery opened and we get gastroenterology and surgery consultations to talk about the management of her acute cholecystitis with the recent myocardial infarct. 04:53 She gets intravenous antibiotics to control the infection in the gallbladder and then we have a number of options; one the radiologist could put a tube in and a drain the gallbladder and wait a few weeks cuz surgeons don’t like to operate on people who’ve had a recent heart attack, a recent myocardial infarct. 05:13 On the other hand, one could do laparoscopic cholecystectomy which is much less traumatic and could be done very, very, quickly. Some people would argue the best option was laparoscopic, some people would say drainage followed by laparoscopic down the road. 05:27 In any case, her gallbladder has to come out because one’s it’s been infected like this there’s a high likelihood that this will happen again.
About the Lecture
The lecture Cardiac Case: 62-year-old Woman with Fever and Epigastric Discomfort by Joseph Alpert, MD is from the course Cardiovascular Cases.
Included Quiz Questions
Which of the following would be the most direct sign of increased right atrial pressure?
- Increased JVP
- Hypotension
- Bradycardia
- S3 heart sound
- Aortic stenosis
ST-segment depression indicates which of the following?
- Myocardial ischemia
- Second-degree AV block
- Atrial flutter
- Ventricular fibrillation
- Transmural myocardial infarction
Author of lecture Cardiac Case: 62-year-old Woman with Fever and Epigastric Discomfort

Joseph Alpert, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Dr. Alpert provides such a clear & concise overview about high-yield diagnosis & management strategies! Thank you for creating this very helpful lecture series!
