Playlist
Show Playlist
Hide Playlist
Cardiac Amyloidosis, Endomyocardial Fibrosis, and Loeffler Endomyocarditis

-
Slides Cardiomyopathy.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
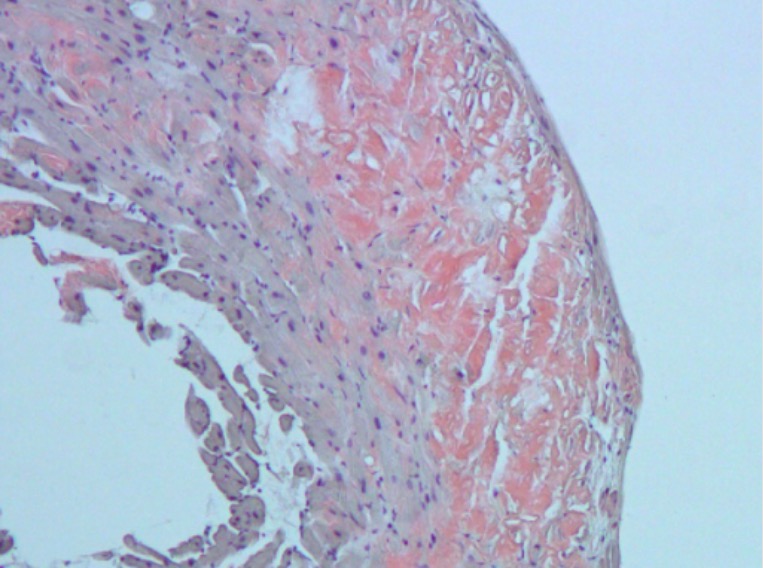
00:01 The most common cause of restrictive cardiomyopathy is cardiac amyloidosis. 00:05 So this is an extracellular deposition of proteins and there are a variety of proteins that can form amyloid. 00:11 Amyloid is any of a variety of proteins that will form insoluble beta pleated sheets that's just demonstrated there on the right, so it kind of looks like a corrugated tin roof. 00:23 And that material can then undergo non-enzymatic crosslinking which makes it very insoluble, and that can accumulate over time and compress and basically make for a very stiff wall. 00:36 The most common cause of amyloid-associated cardiomyopathy is going to be transthyretin. 00:43 That's the protein, and it's interesting, it's produced by the liver. 00:47 Its normal function is to transport thyroxin, and retinal hence the name Trans-thy-retin. 00:55 So you can remember that. 00:56 It's a normal protein, and we make it our entire lifetime. 01:01 But what happens as you get older and older and older, into the 70s, 80s and 90s, you don't break it down. 01:08 And probably because of the nature of the normal extracellular matrix within the myocardium, you get a deposition of this protein that then undergoes non-enzymatic cross-linkage and leads to the deposition, increasing amounts of the amyloid protein. 01:25 We can also see amyloid deposition due to other proteins. 01:30 Transthyretin just happens to be the most common in the aged population, but if a patient has multiple myeloma, and is making abnormal amounts of light chain, light chains can also deposit as an AL, amyloid light chain type amyloidosis. 01:48 Besides depositing it as amyloid, it turns out that light chains are also directly cardiotoxic. 01:55 So in very early amyloid deposition, may actually even have somewhat of a dilated cardiomyopathy due to the toxic nature of amyloid light chains. 02:06 Predominantly,this overload of amyloid can be in multiple tissues. 02:14 In fact, if we see it in the heart, we'll also find it to some extent in lung and we can find it in valves and we can find it in other tissues. 02:21 But the symptomatology of this transthyretin, the senile cardiac amyloidosis, the symptomatology is related to effects due to deposition of the amyloid in the heart. 02:34 Interestingly, you can have normal forms of transthyretin that deposit as you get older and older, because you're just not breaking them down as effectively, or you can have mutant forms of trans they written that deposit. 02:47 And interestingly, in the African American population, roughly 4-5% of that group carry specific mutations that increase the risk of amyloid deposition, and they will tend to have amyloid accumulating at a younger age, say 60 to 70. 03:04 What does it look like? The darker pinker cells that you see there represent normal cardiac myocytes. 03:12 That lighter pink material in between is the amyloid deposition. 03:17 So I kind of like to think about this as pavement stones with mortar in between and the mortar being the amyloid, you can see that that forces the cardiac myocytes apart, so that they don't have really normal connections to each other. 03:32 So they may be prone to arrhythmia, but by having this stiff material that is not contractile, you end up with a restrictive cardiomyopathy. 03:42 The classic study that one does to confirm on histology that you have amyloid deposition is a Congo red stain, and that will appear on the boards. 03:52 It's just one of those things that they like to ask. 03:55 It's an easy one to remember. 03:56 You know, it's just Congo red for amyloid. 03:59 When you shine polarized light on this, the Congo red molecules will they’re in a kind of crystalline array to the amyloid and you shine polarized light and they bend it in a refractile way and we get an apple green, which is indicated there birefringence. 04:18 Okay, so that's, that's the classic histology for cardiac amyloidosis. 04:25 Let's step away from the geriatric population with senile cardiac amyloid and talk about the pediatric population. 04:31 So in that group, the most common cause of restrictive cardiomyopathy is going to be endomyocardial fibrosis. 04:38 This occurs mainly in certain geographical regions, tropical and subtropical regions can affect the valves in addition to thickening the endocardium and making for a stiffer endocardial surface. 04:54 We don't really understand the pathogenesis of this. 04:58 Possible things that have been implicated in nutritional deficiencies, such as inadequate magnesium. 05:05 There may also be parasitic infections leading to hypereosinophilia. 05:09 And in the moment, we'll talk more about increased eosinophils causing endocardial fibrosis. 05:15 So maybe that's one of the components of this pediatric endomyocardial fibrosis. 05:20 Unclear. 05:22 Certain viral infections can also lead to this endocardial fibrosis and exposure to certain elements, certain compounds, so cerium for example, These are all implicated, none of them are proven. 05:38 We just see this in a particular population and we typically see it in again the tropical and subtropical regions. 05:46 This is to be compared and contrasted with the adult, mostly adult form of endocardial fibrosis. 05:55 This is Loeffler's endomyocarditis, so it is an inflammation of the endomyocardium predominantly, named after the physician who first described it Dr. Loeffler. 06:06 As opposed to the endocardial fibrosis associated with little kids, there's no geographic or population predilection,but what is associated with it as shown on the right, lots and lots of eosinophils. 06:17 So there is typically not exclusively not always, but there's often peripheral eosinophilia, being elevated eosinophils in the peripheral blood, and what we will see as the driving force, eosinophilic infiltration of various tissues and particularly of the endocardium. 06:37 So, as we are getting eosinophilic degranulation and damage to the endocardial surface due to these eosinophils, we are causing endothelial damage, and we will tend to get than large mural thrombi that then also organize to form increasing thickness of theendocardium. 06:58 Potentially for some forms of Loeffler endomyocarditis, those that may actually have a low grade malignancy potential, tyrosine kinase inhibitors can help. 07:09 They are not helpful in all cases. 07:12 So, the pathogenesis here, it's hypereosinophilia and it can be malignant or premalignant hematologic disorders such as acute promyelocytic leukemia. 07:22 It can be allergic and autoimmune diseases, again, other causes of increased peripheral eosinophilia. 07:28 It can be certain infections that drive an eosinophilic response in particular, many parasites, some helminths, some protozoa. 07:37 You get an eosinophilic infiltration of the endocardium, and there they release their granules, major basic protein and others causing endothelial and endocardial damage. 07:48 And as a result of that, you get then this fibrosis. 07:52 And because of the damage to the endothelium,you get layering of thrombus and as that organizes, then you get more thickening of the walls. 08:03 Combination of the fibrosis and the organization of the thrombus leads to a very thickened and non-contractile endocardial surface, and hence a restrictive cardiomyopathy. 08:13 And with that, we've covered a rather broad range of topics. 08:17 Hopefully you now have a better way of thinking about dilated, hypertrophic and restrictive cardiomyopathy.
About the Lecture
The lecture Cardiac Amyloidosis, Endomyocardial Fibrosis, and Loeffler Endomyocarditis by Richard Mitchell, MD, PhD is from the course Cardiomyopathy.
Included Quiz Questions
What best describes the pathophysiology of cardiac amyloidosis?
- There is an extracellular deposition of proteins forming beta-pleated sheets that stiffen and restrict the heart.
- There is an intracellular deposition of proteins forming beta-pleated sheets that stiffen and restrict the heart.
- There is an extracellular deposition of proteins forming alpha-pleated sheets that stiffen and restrict the heart.
- There is an intracellular deposition of proteins forming beta-pleated sheets that cause electrical conduction abnormalities.
- There is an extracellular deposition of proteins forming beta-pleated sheets that cause electrical conduction abnormalities.
What is seen after applying a Congo red stain to heart tissue with cardiac amyloidosis?
- A Congo red stain produces apple-green birefringence under polarized light.
- A Congo red stain produces dark-red birefringence under polarized light.
- A Congo red stain produces reactive oxygen species.
- A Congo red stain does not produce any distinctive pathological features in tissue with amyloid deposits.
- A Congo red stain produces violet birefringence under polarized light.
What is a potential cause of endomyocardial fibrosis?
- Hypereosinophilia
- Fungal infection
- Exposure to arsenic
- Exposure to radon
- Cigarette smoking
What is true about Loeffler endocarditis?
- It is caused by a parasitic infection.
- There is a predilection for hot, humid climates.
- It is associated with deep vein thrombosis.
- It is associated with a bacterial infection.
- There is a predilection for cold, dry climates.
Author of lecture Cardiac Amyloidosis, Endomyocardial Fibrosis, and Loeffler Endomyocarditis

Richard Mitchell, MD, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
