Playlist
Show Playlist
Hide Playlist
Carcinoid: Diagnosis and Management

-
Slides CarcinoidSyndrome Surgery.pdf
-
Download Lecture Overview
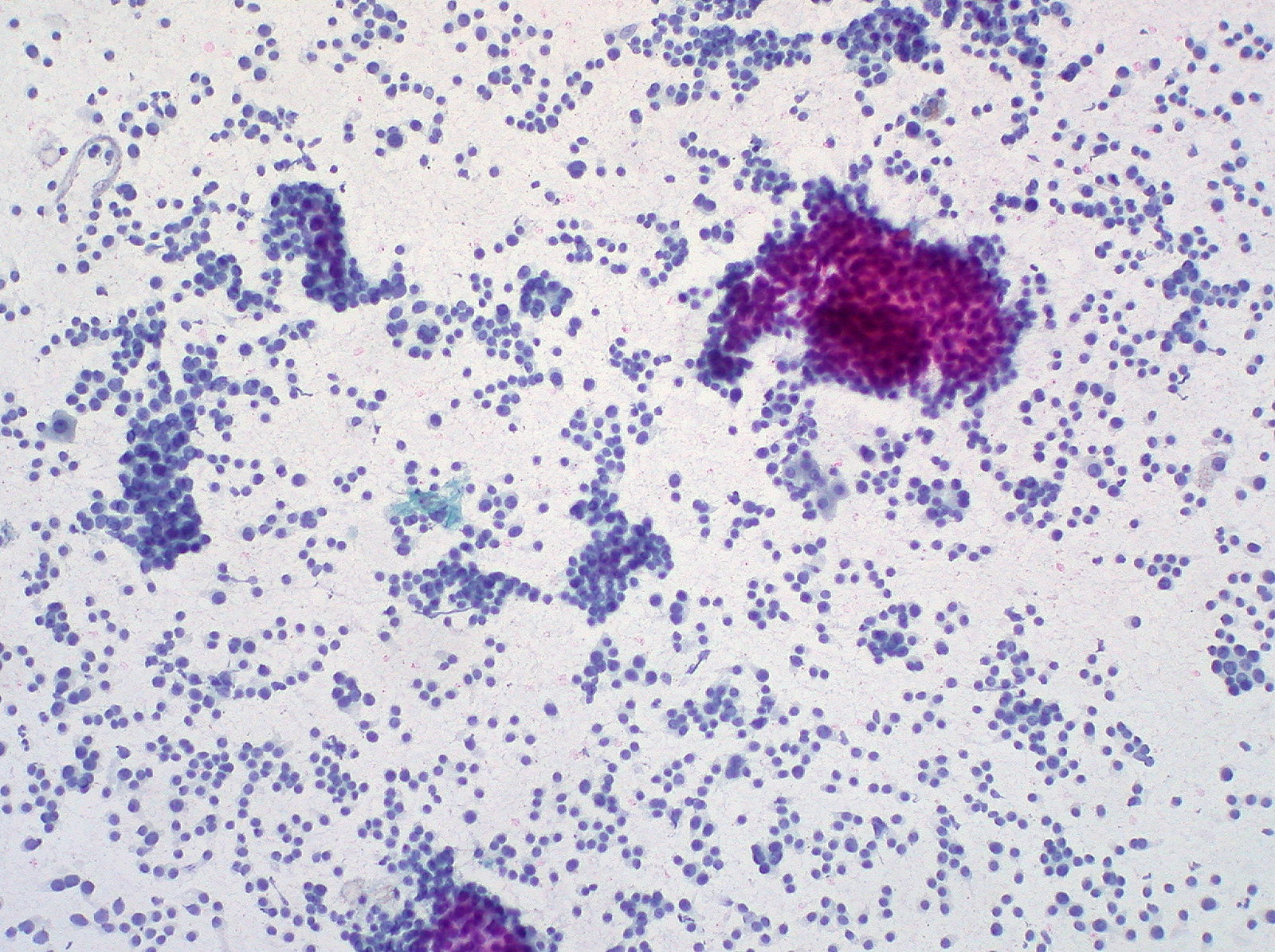
00:01 Traditional labs may not be very helpful. This includes the chemistry or the CBC. To diagnose an increase in serotonin secretion, we collect a 24-hour urine 5-HIAA as well as a plasma chromogranin A level. 00:21 What’s chromogranin A? Neuroendocrine tumor vesicles secrete chromogranin A which is very specific for neuroendocrine tumors. It is not dependent on serotonin secretion making it very, very ideal for our diagnosis. It is more sensitive but less specific unfortunately than 5-HIAA. Recall 5-HIAA is a metabolite of serotonin. Plasma levels correlate well with the treatment response. It’s important after treatment of neuroendocrine tumors to follow the chromogranin A level. And it may have prognostic value. Here’s an axial cross-sectional CT demonstrating potential locations of carcinoid tumor. You’ll notice in the highlighted circles areas of the small intestines that may contain the tumor. 01:20 Sometimes, octreotide scans are also helpful to delineate where exactly the carcinoid tumor may be. At surgery, if it was in a small bowel carcinoid with no metastasis, this is what we would do, a segmental small bowel resection. You’ll notice from this image that a segment of small intestines has been removed or placed out of continuity. The remainder of the small bowel will be put back together either in a hands-on or a stapled manner. Here’s what a carcinoid tumor might look like in the actual small intestine specimen. Very important discussion about liver degradation: Remember my discussion about how metastasis is very important in the development of neuroendocrine tumor or carcinoid tumor symptoms? The reason is this. Vasoactive peptides are usually degraded by the liver. 02:14 However, when these vasoactive peptides overwhelm the liver degradation, this implies that the primary tumor has spread beyond the liver or beyond the liver’s ability to degrade the vasoactive peptides. 02:27 Only when the carcinoid tumor spreads beyond the liver do patients become symptomatic. Important clinical pearls: Carcinoid tumors are largely well differentiated and indolent tumors. Most carcinoid tumors do not lead to the carcinoid syndrome. Our liver have extreme protective mechanisms and they will degrade the vasoactive peptides. High-yield for examination: Symptoms of carcinoid syndrome, just as a reminder, flushing, cardiac complications, tricuspid regurgitation, abdominal pain, all imply a spread to the liver. Bronchial tumors can cause carcinoid syndrome because of direct secretion to the systemic circulation. Again, if the tumor was in the bronchial system or the lungs, the liver has not had the chance to degrade the vasoactive peptides. The serotonin can then directly go into the systemic circulation. For patients who have bronchial tumors, their symptoms may occur earlier than those who had GI carcinoid tumors. Thank you very much for joining me on this discussion of carcinoid syndrome.
About the Lecture
The lecture Carcinoid: Diagnosis and Management by Kevin Pei, MD is from the course General Surgery.
Included Quiz Questions
Which of the following is NOT true about chromogranin A levels?
- It is more specific when compared to 5-HIAA.
- It is more sensitive when compared to 5-HIAA.
- It is not dependent on serotonin secretion.
- It is secreted by neuroendocrine tumors.
- It may have prognostic value.
A patient presents with flushing, asthma-like symptoms, and weight loss. Which of the following is NOT included in the differential diagnosis?
- Localized early carcinoid tumor in the duodenum
- Localized early carcinoid tumor in the bronchi
- Metastatic carcinoid tumor to the brain
- Metastatic carcinoid tumor to the lungs
- Metastatic carcinoid tumor to the liver
Author of lecture Carcinoid: Diagnosis and Management

Kevin Pei, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
