Playlist
Show Playlist
Hide Playlist
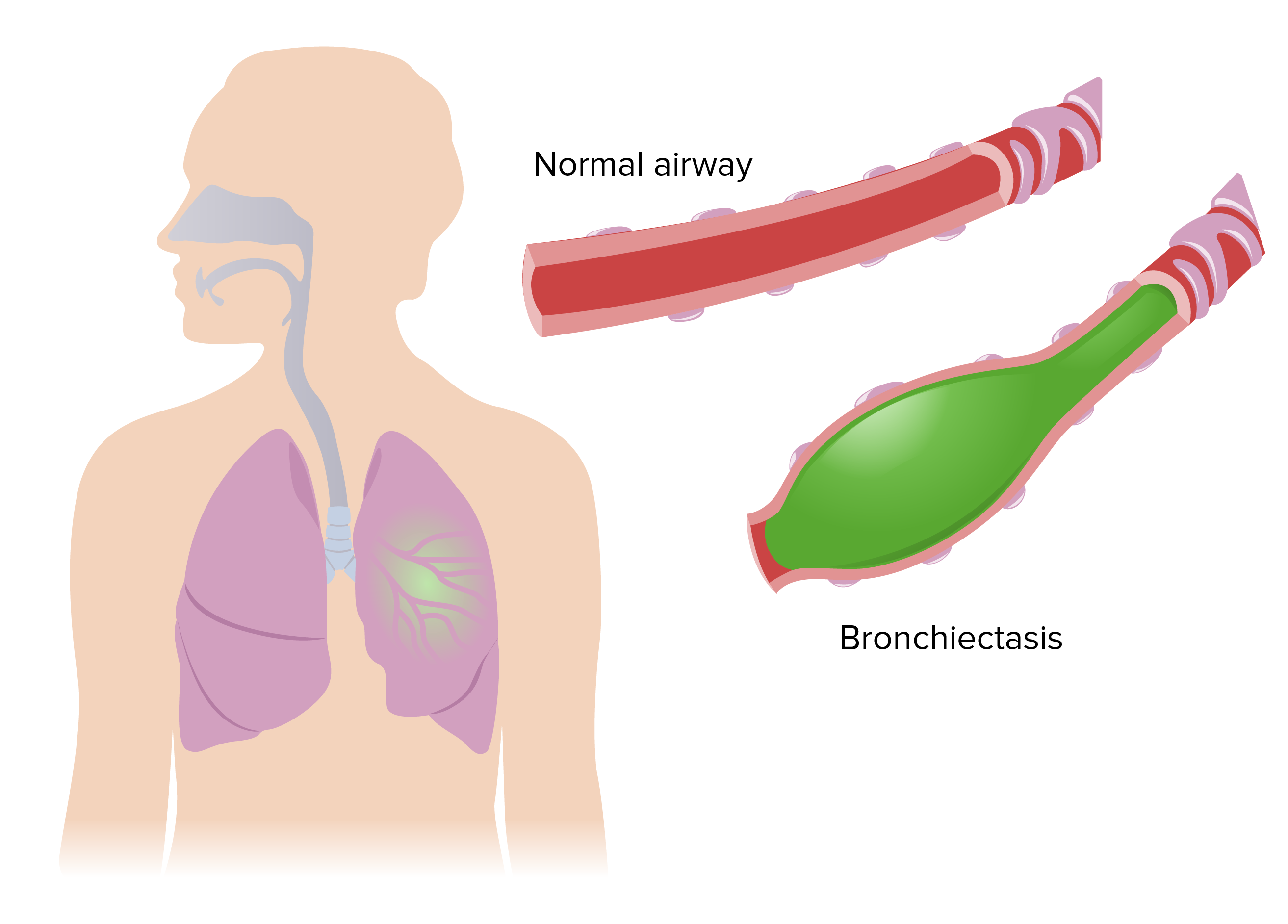
Bronchiectasis: Presentation and Clinical Signs

-
Slides 05 MajorAirwaysObstructionBronchiectasis RespiratoryAdvanced.pdf
-
Download Lecture Overview
00:01 So how do patients present with bronchiectasis, well the common types of presentation include the following - One, it is a daily production of purulent phlegm. So that could be a small amount, a teaspoon of green gunky phlegm per day or it could be as much as a cup or even more per day with more severe disease. Now that's a marker of patients who really do have active bronchiectasis with quite significant anatomical damage. The less marked disease, the less severe disease patients may not have daily purulent sputum production but will have acute attacks of exacerbations whether they produce green phlegm for a few days that respond to antibiotics and makes them feel better, but these keep coming back. Most patients, most people do not get too many chest infections in their life, if you're getting chest infections every year or several times a year, that should raise the suspicion that the patient has a bronchiectasis unless they have an underlying other lung disease such as COPD, or are they known to smoke. Similarly sputum's cultures are not normally positive in normal people repeatedly, so if you keep identifying bacterial organisms which are known to be pathogens such as Haemophilus Influenzae, Morexalla, Streptococcus pneumoniae or Staphylococcus aureus from sputum samples in an individual then you need to think that they might have bronchiectasis and Pseudomonas aeruginosa is a bacteria which only normally colonizes abnormal lungs, so if you isolate that in sputum, you really need to think about bronchiectasis diagnosis. Aspergillus is found in the lungs of patients with allergic bronchopulmonary aspergillosis, and again if you culture it, therefore you need to think about bronchiectasis and ABPA as a diagnosis. Bronchiectasis is one of the major causes of hamemoptysis, so an episode of major hemoptysis or repeated episodes of minor hemoptysis might suggest bronchiectasis. The signs of bronchiectasis are coarse crackles and somebody always has coarse crackles in the same area of the lung whenever you listen to them, then again that would suggest that there's some damage there and bronchiectasis is one of the possible causes. And finally, with a CT scans being used frequently nowadays for accessing patients with lung disease of various different types, then bronchiectasis is often identified. For example in my clinic I frequently see patients with being referred from the two week wait clinic where patients have been referred from investigation for an abnormal X ray because people are worried they may have cancer, but it turns out the abnormality on the X ray is due to bronchiectasis. Right, so common associations of bronchiectasis, what other problems do patients of bronchiectasis have? Well, they often have asthma, some reversible airways obstruction, that’s the patients with the mild forms of bronchiectasis. 02:45 The more severe forms of bronchiectasis, as I’ve already mentioned leads to irreversible airways obstructions, you get small airways obliterative bronchiolitis and that is the mechanism by which bronchiectasis causes patients to develop respiratory failure and causes death. 03:01 Patients with bronchiectasis, specifically the idiopathic patients and those with mucociliary clearance problems such as cystic fibrosis, they frequently have rhinitis, sinusitis, middle ear disease, so upper airway problems as well. Occasionally patients with bronchiectasis will have infertility, that’s an example of mucociliary clearance problems, affecting sperm production as well, and infections with non-tuberculosis mycobacteria are problems as well. How do you recognize clinically on examination patients? Combination of clubbing and coarse crackles within the lung. Actually clubbing is pretty rare unless the patient has severe or aggressive disease. The crackles though, are usually present in patients with bronchiectasis, and they can be accompanied by the squeaks and by wheeze of the airways obstruction, and when the patients have really bad bronchiectasis they will develop the signs of severe airways obstruction as well, the similar signs that we described in COPD.
About the Lecture
The lecture Bronchiectasis: Presentation and Clinical Signs by Jeremy Brown, PhD, MRCP(UK), MBBS is from the course Airway Diseases.
Included Quiz Questions
Which of the following best describes the classic clinical manifestation of bronchiectasis?
- Daily cough with mucopurulent and tenacious sputum lasting months to years
- Dry cough lasting days to weeks
- Progressive dyspnea and cough with rales in a heavy smoker who is elderly
- Cough with sputum expectoration for at least 3 months a year during a period of 2 consecutive years
- Chronic productive cough with hemoptysis
Author of lecture Bronchiectasis: Presentation and Clinical Signs

Jeremy Brown, PhD, MRCP(UK), MBBS
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
