Playlist
Show Playlist
Hide Playlist
Brain Herniation

-
Slides 05 IncreasedIntracranialPressure Neuropathology I.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
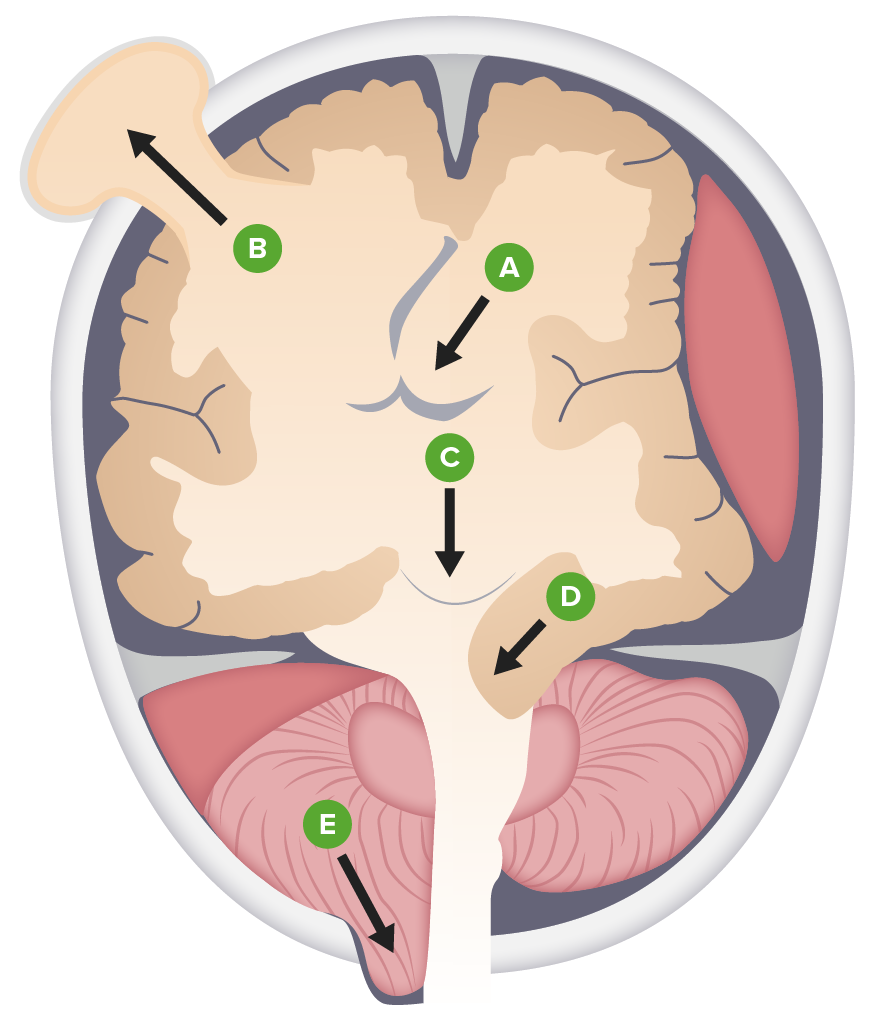
00:01 Let’s talk about subfalcine quickly. 00:03 We call this a cingulate gyrus. 00:05 What’s happening? You’re going underneath the falx cerebri to the opposite side. 00:09 What are you doing? You are hurting or compressing the branches of the anterior cerebral artery. 00:16 And my problem is going to be where? Upper or lower extremity, please? Lower extremity. 00:21 Let’s move on. 00:22 Transtentorial, where are you? Medial temporal lobe. 00:28 And this is known as your uncus. 00:30 We call this transtentorial or uncal herniation. 00:34 What is it doing? This temporal lobe or herniation is then going to cause compression of perhaps the third cranial nerve. 00:41 That’s your oculomotor. 00:43 If you lose your parasympathetic, what may happen to the pupil? Good. 00:47 Blown. 00:48 Mydriatic. 00:49 Why? Because you lose the parasympathetic. 00:53 One more time, what if the papillary constriction is intact? And you only have a motor issue with oculomotor. 01:01 There must be infarction to that nerve. 01:04 Example, diabetes. 01:06 I’ve mentioned that before, I’m mentioning it now. 01:08 If you’re not familiar with it, please make sure that you divide the oculomotor into compression effects with pupillary compromise or papillary functioning intact, which would then refer to your infarctions. 01:23 In addition, temporal lobe compressed against the tentorium cerebelli. 01:27 There’s every possibility that you not only have an uncal herniation, but then at the same time, you could have a tonsillary herniation. 01:34 What is your tonsil referring to once again? It’s the cerebellar tonsils that are then herniating into the foramen magnum. 01:40 Compression of the medullary respiratory center. 01:43 Look for that. 01:45 That’s your tonsillar herniation. 01:47 One thing that I want to bring to your attention is that if there’s an uncal herniation and you’re pressing upon that brain stem and you’re pushing it downwards, you might then cause stretching of the vessels of the brain stem, aren’t you? Stretching of the blood vessels of the brain stem. 02:02 What if it ruptures? What do you call this? What kind of hemorrhage is this? A Duret hemorrhage. 02:08 D-U-R-E-T. 02:10 Duret hemorrhage. 02:12 Beautiful story, isn’t it? All under the premise of increased intracranial pressure. 02:19 Management. 02:20 Simple measures make all the difference in the world. 02:23 Raise the bed for 45 degrees, try to drain the fluid conservatively. 02:28 And that is an answer choice. 02:31 No circumferential tape around the neck for securing your ETT. Your endotracheal tube. 02:37 So that you dont increase your jugular venous pressure. 02:40 Hyperventilation. 02:42 Simple measures. 02:43 PCO2 normally should be at 40. 02:46 Hyperventilation will then cause your blowing off your carbon dioxide and it starts dropping below 40. 02:53 This could help with simple measures of the decreasing intracranial pressure. 02:59 Or mannitol. 03:00 What does mannitol mean to you? It’s a huge osmotic drug. 03:05 And this osmotic agent is going to do what? Simple measures to decrease intracranial pressure. 03:11 It brings about drainage because it’s an osmotic agent, is that clear? Don’t worry about the dosage so much right now. 03:18 Simple measures. 03:19 Any one of these could be answer choices. 03:21 Use common sense. 03:23 Now, apart from that, you get a little bit more invasive. 03:28 You want to be careful. 03:30 So mannitol did what? It was an osmotic agent that was pulling water out. 03:36 What kind of saline might you want to use so that you can have the same type of effect please? Good. 03:41 Greater than 0.9%, right? Normal saline is 0.9%. 03:46 Maybe using 1, 2, or 3%. 03:49 A "bullet" 30 cc’s. 03:51 IV steroids if due to a tumor and at some point maybe a catheter or intraventricular type of drainage. 03:58 You go from simple measures and you start getting into what you need to do so that you can drain some of these fluid to decrease the intracranial pressure. 04:06 In the meantime though, you’re always going to look for what is the underlying cause in the skull, the brain in the box, remember? And what’s in that box? You could have the brain itself. 04:15 You could have the blood. 04:16 You could have the CSF. 04:17 And anyone of those could result in increased intracranial pressure. 04:20 In the meantime, you need to make sure that you make the patient feel comfortable. 04:24 Otherwise, we got issues.
About the Lecture
The lecture Brain Herniation by Carlo Raj, MD is from the course Increased Intracranial Pressure (ICP). It contains the following chapters:
- Herniation
- Increased Intracranial Pressure: Treatment
Included Quiz Questions
Which type of brain herniation can cause death due to compression of the respiratory centers?
- Tonsillar herniation
- Cingulate gyrus herniation
- Transtentorial herniation
- Uncal herniation
- Cerebral herniation
What is a simple measure that can help a patient with increased intracranial pressure?
- Raising the head of the bed by 45 degrees
- Administering IV heparin
- Loop diuretics
- Blood pressure control
- Hypoventilation
Author of lecture Brain Herniation

Carlo Raj, MD
Customer reviews
3,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
1 |
clear and exactly what is needed from subfalcine herniation. continue to provide these great lectures!
Just reading from the slide not explaining anything at all. Could really use some illustrations to differentiate the different types of brain herniation.
