Playlist
Show Playlist
Hide Playlist
Bradycardia (Slow Heart Rate)

-
Slides Alverson Arrythmias in children.pdf
-
Reference List Pediatric Nursing.pdf
-
Download Lecture Overview
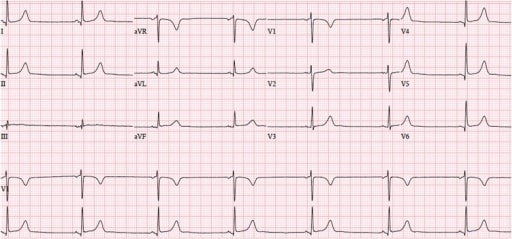
00:01 In this lecture, we're going to review the basics of arrhythmias in children. 00:06 Let's start with bradycardia -- when the heart is going too slow. 00:11 Now in children as opposed to adults, there is variability on what is considered a normal heart rate. 00:18 This is because infants typically have a much higher heart than adults, and gradually the heart rate slows down as we age. 00:25 In infants, bradycardia is considered any heart rate less than 100 beats per minute. 00:31 In young children, we lower that number to about 60 beats per minute, and in older children we typically say bradycardia is less than 50 beats per minute. 00:41 However, I will say there are quite a few children who will present to the hospital and be admitted overnight for something unrelated to their heart, and have a transiently low heart rate in the 40s with a normal blood pressure. And as long as they're doing well, we'll consider that within the normal amount of variation. 00:58 It's rare but it's absolutely possible. 01:01 So before we start talking about abnormal causes of bradycardia in children let's review briefly the electrical conduction system of the heart. 01:11 The heartbeat is generated in the sinus node. 01:14 It's transmitted through internodal pathways to the AV node which then sends the signal down the bundles up to the Purkinje fibers and into the ventricular muscle. 01:26 So, bradycardia can originate at several different places throughout the system. 01:32 Let's start with bradycardia originating at the SA node. 01:36 The SA node is controlled by external factors in the body, such as the vagus nerve. 01:44 So, the SA node is what really determines the rate of heartbeat in a normal individual. 01:51 Things that slow things at the SA node are things such as medications; a beta-blocker for example would cause sinus bradycardia. 02:00 Now, we think of beta-blockers as being a medication we would give for this very purpose, but children are difficult and sometimes two-year-olds can get into mom's medications and show up with an abnormal bradycardia -- they happen to have eaten mom's beta-blocker. 02:17 Another possibility is just increased vagal tone. 02:20 For some reason that child may have increased vagal tone. 02:23 It may be a baseline condition or maybe a result of something else. 02:27 Or, and this we actually see sometimes as increased intracranial pressure, or ICP. 02:32 Children with, for example, hydrocephalus may present with bradycardia. 02:37 So, if you suspect then slowing at the AV node, there are several different types we should go through: First, second, and third degree heart block, and there's two in the second-degree that we should discuss. 02:50 Let's start with first degree heart block. 02:53 First degree heart block is a prolongation of the PR-interval on an EKG. 03:00 It's a delay in the time between the atrial contraction and the ventricular contraction. 03:06 This is an EKG with a patient with first degree heart block. 03:10 If we zoom in really close, we can see that there's a longer distance than normal between the P wave and the subsequent QRS. 03:18 This patient has first degree heart block. 03:21 Now, in second degree heart block, it's going to be a changing system. 03:27 So, in the first type of second degree heart block which is called Mobitz Type 1, and it's also called "Wenckebach block," you have a gradual prolongation of the PR-interval until the beat just gets missed entirely. 03:44 So as you can see here, we have the first beat which has a prolonged PR-interval; the second beat which has a very prolonged PR-interval; and then where the third beat should have happened, the PR-interval was so long the beat just got dropped and then the system resets again. 04:01 And you'll sometimes see many of these within the same EKG. 04:04 So, that's Mobitz Type 1 or Wenckebach block. 04:07 Mobitz Type 2 is a little bit different. 04:11 Here's a drawing of a Mobitz Type 2. 04:14 Here, the PR-intervals are all prolonged at the same amount, but then the beat simply gets dropped. 04:21 So, that's Mobitz Type 2. 04:25 The third degree heart block is a little bit different. 04:28 And here what we have is a complete dissociation of the atrial beats and the ventricular beats. 04:35 Let's walk through this together. 04:36 Here you can follow some P intervals or P waves as they're marching along an EKG. 04:42 There's one, there's one, there is one, there is one, there is one. 04:47 These are occurring at regular intervals, but their intervals are very different than the QRS complexes. 04:54 The QRSes are marching out here, here, and here. 05:00 This child essentially has two heartbeats. 05:03 They have the atrial heartbeat, which you really can't palpate because the atria don't do much in terms of providing circulation and pressure on the pulse; and the ventricular heartbeats which you can feel. 05:15 So, this patient will present with bradycardia and a complete dissociation of P waves and QRSes on their EKG. 05:23 How do patients with bradycardia typically present? Well, they may present with a sensation of palpitations. 05:31 Oftentimes that's because beats are getting dropped and that feels uncomfortable. 05:36 They may present with dizziness. This is because they aren't capable of raising their heart rate under times when you would need extra perfusion. 05:44 For example, if I stand up suddenly, I need to generate more pressure to perfuse my brain. 05:49 If I have a problem with my PR-interval I might not be able to raise my heart rate entirely to accommodate that extra-needed blood pressure, I'll feel dizzy and woozy. 06:00 And they may have so much dizziness that they frankly have syncope. 06:04 So, if we suspect bradycardia in a patient, the obvious thing is we're gonna get an EKG and that's really gonna help us make our diagnosis. 06:13 There are times, however, when patients come in and out of bradycardia or they're having some symptoms sometimes but not others, and that's when we might do something like 24-hour Holter monitoring. 06:25 24-hour Holter monitoring is really clever. 06:27 It's a machine, a device that the patient carries with him for a day. 06:31 They have a button they could actuate and press if they have feeling symptoms, and it's measuring their heart rate continuously and recording that. 06:38 Then the device is taken to the cardiologist, and the cardiologist can look at the device and see what exactly is going on with the heart at that time. 06:48 There is a special condition in children where children can get very, very severe heart block and it relates to their mother. 06:56 In neonatal lupus exposure, the baby has a mother with lupus. 07:02 While in utero, the mother's lupus antibodies were able to get through the placenta and get to the baby. 07:09 Here on the slide you can see a baby with discoid lupus. 07:13 You can see those round circles that you typically see in adults with lupus. 07:17 The baby does not have lupus; the mother does. 07:21 But the mother's antibodies have crossed the placenta and are creating symptoms of lupus that this baby can have, including the rash, the malar rash which they might have this baby doesn't have it but many do, the baby could have abnormal cell counts, the baby might have arthritis -- all the findings of lupus. 07:39 But one finding in particular the baby might have is bradycardia and complete heart block. 07:45 Infants born to women with lupus are at risk for heart block, and unlike all the other findings which gradually resolve, for this infant the bradycardia will be permanent. 07:56 A pacemaker is required for life.
About the Lecture
The lecture Bradycardia (Slow Heart Rate) by Brian Alverson, MD is from the course Pediatric Cardiology. It contains the following chapters:
- Definition
- Pathology
- Clinical Presentation & Diagnosis
- Neonatal Bradycardia
Included Quiz Questions
An ECG shows regular P waves and wide QRS complexes at regular intervals without any relationship between the P waves and the QRS complexes. Which of the following is the most likely diagnosis?
- Third-degree heart block
- First-degree heart block
- Mobitz type 1 heart block
- Mobitz type 2 heart block
- Left bundle-branch block
Which of the following does not decrease the rate of sinoatrial node pacing?
- Albuterol
- Beta blockers
- Hydrocephalus
- Increased vagal tone
- Sick sinus syndrome
Which of the following is the initial choice of investigation in a patient with bradycardia?
- ECG
- Echocardiogram
- 24-hour Holter monitoring
- Chest X-ray
- Angiography
Which of the following is true about a child with bradycardia born to a mother with anti-Ro-positive lupus?
- It is most likely due to a congenital heart block.
- Bradycardia is most likely transient.
- It rarely requires any treatment.
- It will require immediate surgery.
- The infant should not be breastfed.
Author of lecture Bradycardia (Slow Heart Rate)

Brian Alverson, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
4 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
I really liked the explanation for the different types of heart block!
These are the best explanations regarding bradycardia that I heard of. I would have liked to hear more about other drugs that could cause bradycardia though. That being said, I think that now I cannot forget the different blocks. So thank you very much! Also cool that the case of neonatal bradycardia is talked about.
The AV blocks were explained so clearly. I have never understood the differences between the three types before. thank you
Very easy to understand, high yield points and such a great teacher. Congrats ! =D
