Playlist
Show Playlist
Hide Playlist
Bacteroides

-
01-22 Bacteroides.pdf
-
Download Lecture Overview
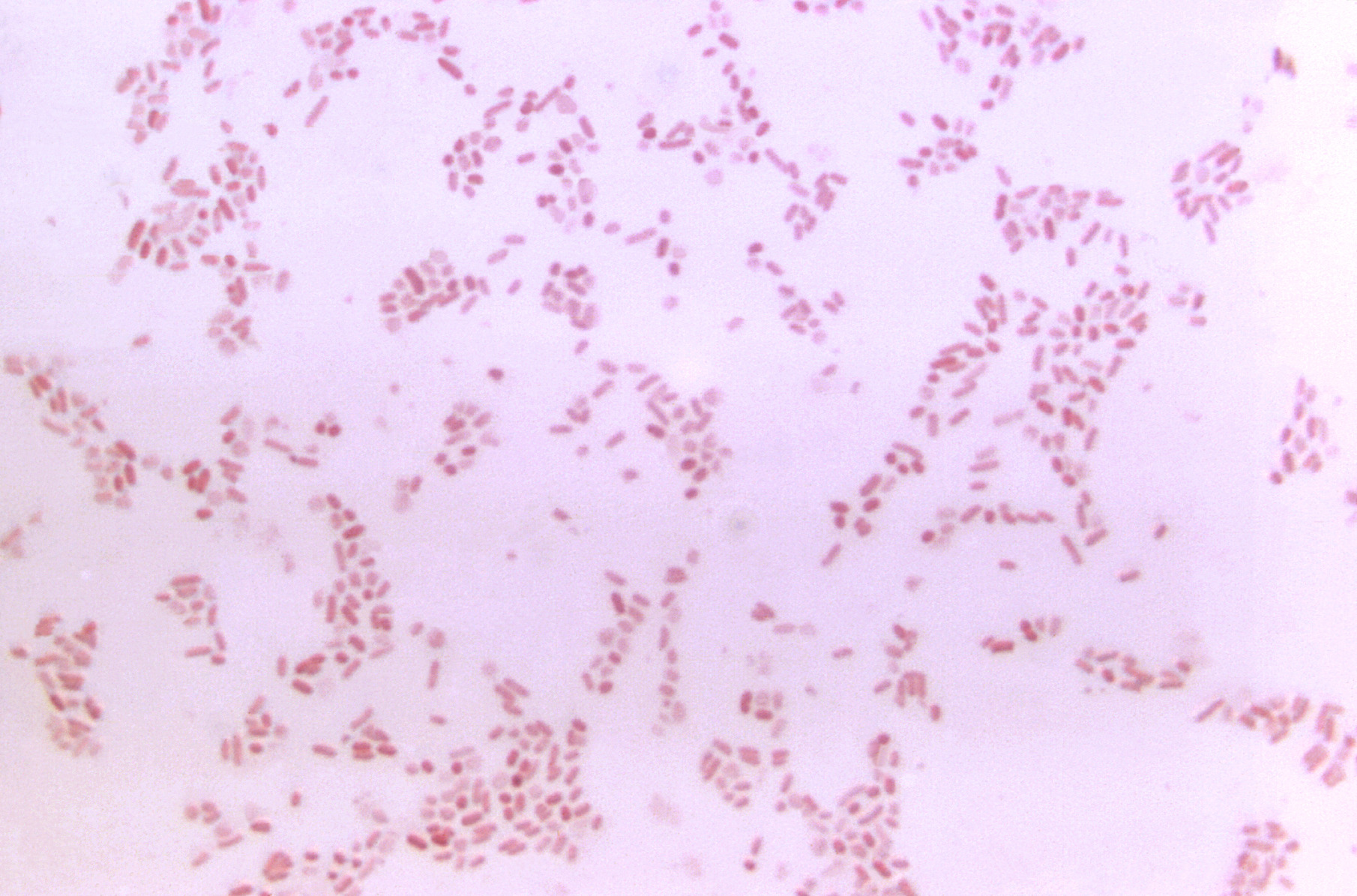
00:01 Bacteroides, a bacteria. 00:04 The Bacteroides are gram-negative, anaerobic, and encapsulated organisms and you can see them on the image projected on the slide. 00:12 These are pleomorphic organisms, again, because they have a somewhat variable staining, a pattern when they’re looked at on the gram stain. 00:19 In addition, they produce very foul-smelling short-chain fatty acids which is one of the signature presentations of a anaerobic infection such as with Bacteroides. 00:31 They have broad antibiotic resistance as we’ll talk about later in this presentation, only a few antibiotics are known to have reliable efficacy against the Bacteroides. 00:43 They do have weak endotoxin activity which contributes to their pathogenesis and unfortunately, they are known to be the normal flora of many parts of the body. 00:53 Respiratory tract, gastrointestinal tract, and the genital urinary tract. 00:58 However, if one were to look at the most common location for the Bacteroides bacteria, it is in the GI tract. 01:06 Think below the diaphragm for presence of Bacteroides. 01:10 The most clinically significant Bacteroides is Bacteroides fragilis and this again, below the diaphragm, an anaerobic cause of gastrointestinal infections. 01:23 The pathogenesis of Bacteroides starts with its capsule in part-- so it is able to allow phagocytosis without death. 01:32 Then, therefore, the Bacteroides combined to peritoneal surfaces after they leave their normal site within the intestines at once binding to peritoneal surfaces can create abscess formation. 01:46 The abscess formation in part is due to the human immune system’s attempt to phagocytose unsuccessfully, the organism itself and then, leading to innocent bystander damage to the surrounding normal cellular tissue. 02:03 Surgery and trauma only accentuate the problem because they can disrupt the abscess itself, allowing the organism to then enter the bloodstream and/or lymph structures and disseminate freely. 02:17 As the dissemination occurs, as the Bacteroides is now getting free access to the rest of the body, it releases further enzymes which can cause tissue destruction. 02:27 So, basically, a very significant enteric pathogen that is just fine until you disturb its normal habitat via surgery or via trauma. 02:37 The infections caused when that happens are typically multiple intraabdominal infections with abscess formation. 02:45 Those can extend into the pelvis to cause abscesses or suppurative pelvic infections and as they disseminate causing entrance into the bloodstream, a bacteremia or a septicemia. In some cases where the intraabdominal infections and abscesses are extensive, they can cause a reactive pleural effusion, so, an effusion within the lung cavity between the lungs, the pleura, and the chest cavity, and that effusion because it is proteinaceous can become secondarily infected. 03:19 So, one can see infections extending from the abdomen to above the diaphragm to cause pleural pulmonary infections. 03:28 Prevention and treatment, well, if one knows that one is going in to do an intraabdominal surgical procedure, in fact, many surgical procedures, there is known violation of normal tissue boundaries of skin integrity, the normal defense mechanisms which the human body has against bacteria and if one knows especially that intraabdominal surgery’s going to occur and has the potential to open up intestinal contents, then, prophylactic antibiotics are indicated, specifically, targeting the bacteria which normally live in the gut. 04:07 Once though an infection has become established, then, removal, surgical removal of necrotic material, purulent material, drainage of abscesses is critically important because antibiotics by themselves will be relatively ineffective, not effective in treating bacteria in the middle of an abscess. Why might this be? Several reasons, number one, antibiotics don’t have a delivery mechanism to the inside of an abscess cavity. 04:37 There’s no blood supply to deliver them into the abscess. 04:41 Thus, they would have to diffuse in through a concentration gradient which is a slow and completely unreliable process. 04:49 Second though is that within the abscess material itself is a very low pH, a very acidic environment. 04:57 Almost all antibiotics are designed or naturally acquired to function at normal pH of the body. 05:05 So, they don’t work well. The molecular structure disintegrates at too high or too low a pH. 05:13 Thus, even if you could get an antibiotic delivered into an abscess cavity, if it has a low pH, that antibiotic will not be highly effective. 05:22 So, surgical drainage, surgical removal is critical, is essential to actually treat those infections caused by Bacteroides fragilis. 05:32 After the surgical drainage occurs, then, antibiotics using especially metronidazole is the best approach. 05:39 Metronidazole is an antibiotic with excellent anaerobic capabilities and excellent tissue penetration. 05:46 There are many available antibiotic regimens that can be selected based on a patient's medication tolerance, drug adverse effects, or even suspicion for antibiotic resistance in their organism. 05:58 Once the culture and susceptibility tests are completed, then of course, the antibiotics can be adjusted to better target or focus on the patient's known infection. 06:06 One typical combination might be metronidazole and cephalosporin. 06:10 Although single agent drugs such as Chippenham or Chippenham sell acetate and also would work.
About the Lecture
The lecture Bacteroides by Sean Elliott, MD is from the course Bacteria.
Included Quiz Questions
Which of the following features best describes Bacteroides species?
- Anaerobic, gram negative, and encapsulated rods
- Anaerobic, gram positive, and encapsulated rods
- Aerobic, gram negative, and encapsulated rods
- Aerobic, gram positive, and encapsulated rods
- Anaerobic, gram negative, and unencapsulated rods
Bacteroides species are most commonly found in which system of the body?
- Gastrointestinal system
- Reproductive system
- Integumentary system
- Urinary system
- Respiratory system
Bacteroides species are most commonly found below which structure of the body?
- Diaphragm
- Stomach
- Pancreas
- Spleen
- Liver
The presence of which lesion in the abdomen indicates a likely infection by Bacteroides fragilis?
- Abscess
- Hematoma
- Granuloma
- Lipoma
- Fibroma
Author of lecture Bacteroides

Sean Elliott, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
