Playlist
Show Playlist
Hide Playlist
Autosomal Dominant Disease

-
Slides RenalCystrePathology IntegratedRenalPathology.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
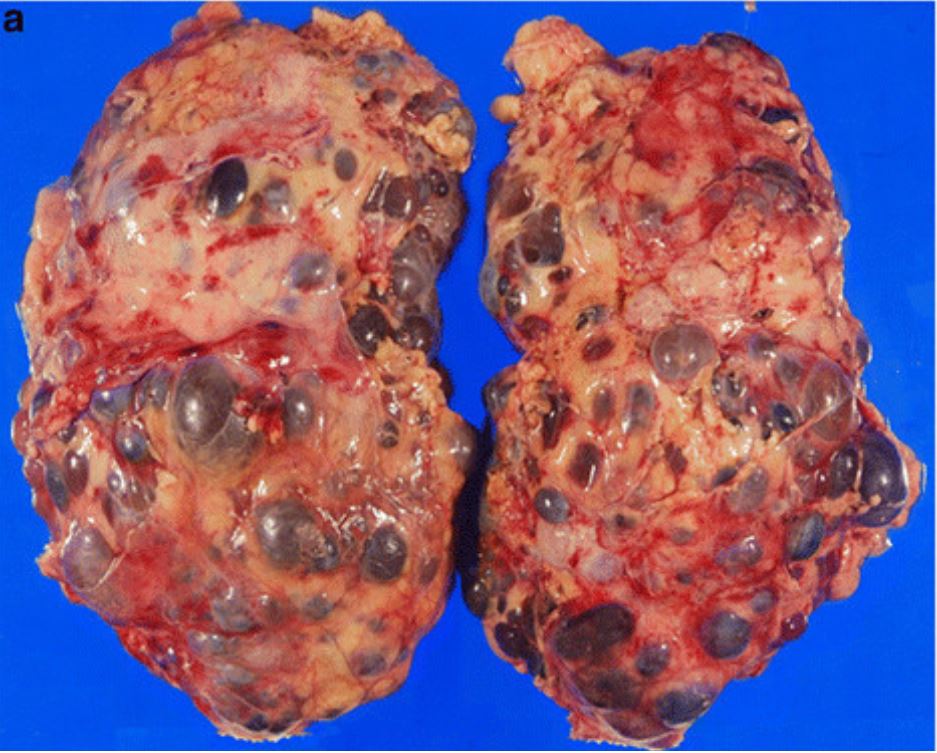
00:01 Let us now move on to Autosomal Dominant. 00:03 Now, a couple of important things about Autosomal Dominant Polycystic Kidney Disease, once upon a time, you might have. And I'm hoping that you haven't. 00:11 So, let's not really even talk about this. 00:14 Apart from the fact that you need to know that it's autosomal dominant. 00:18 Now, the reason that we no longer call this Adult Polycystic Kidney Disease, and I don't want you to do that any longer. 00:25 That's what I was inferring to, is because as far as age groups are concerned, it could be all over the place. 00:31 It could have young patients as well but mostly occurs in adults. 00:35 Autosomal Dominant Polycystic Kidney Disease, I cannot move forward without good conscience without telling you about a very important gene called PKD-1. 00:46 Luckily, ADPKD, Autosomal Dominant Polycystic Kidney Disease, that gene that is seen, 85% of the time with ADPKD is PKD-1. Fantastic. 01:00 That actually works out really well. 01:02 That PKD-1 is important for you to know including chromosome 16. 01:06 Now, PKD-2 is seen in 15% of the time while really, your focus should be on PKD-1. 01:13 Next, Bilateral Cystic Disease developed by 20-25 years of age. 01:18 Now, next important point. 01:20 These cysts that you're seeing in an older patient, well, does that mean that the kidney dies? No. 01:28 Is that clear? At some point, when we go through this table, we'll talk about this patient having ADPKD, and the insidious onset of chronic renal failure. 01:38 So, when you have cysts in the kidney, it does not, I repeat, it does not mean that kidneys are dead. 01:44 In fact, what's the big thing that you're worried about in a patient with ADPKD? Excess renin release. 01:51 Really? Mm-hmm. How is that gonna manifest? You've all heard of Berry Aneurysm, have you not? What's a berry aneurysm? That is a saccular aneurysm taking place most likely, where? In the circle of Willis. 02:05 If that thing ruptures, then your patient has the worst headache, he or she has ever experienced. 02:11 Welcome to subarachnoid hemorrhage. 02:14 Interesting, Autosomal Dominant Polycystic conditions. 02:17 Now, there are a couple of other important side effects, not so much side effects, sequelae that we'll take a look at with ADPKD. 02:24 All parts of nephron are involved. 02:27 Bilaterally, once again, here, not only could you have cysts in the kidney. 02:32 I told you earlier that when you do have cysts in the kidney, oftentimes, you will find it in your liver, no exception here. 02:38 However, this is an adult or older. 02:41 What do you know about your liver? Oh, incredibly resilient, isn't it? Yes, it is. 02:47 It's responsible for quite a bit of taking care of your toxicities including ammonia. 02:52 It's a huge detoxifier of drugs as you know and conjugates. 02:56 It is extremely resilient even to the point where it will regenerate. 03:01 So, as we get older and say that we introduce enough damage to the liver. 03:05 Is it possible than an adult that maybe Congenital Hepatic Fibrosis, that we saw occurring in Autosomal Recessive Polycystic Kidney Disease is not seen here? Yes, very much so. 03:20 So, here when we talk about Congenital Hepatic Fibrosis and Portal Hypertension, that would be more about ARPKD or juvenile. 03:28 Here, could you find it? Sure. But as I said, look for cysts in the liver. 03:33 Pancreas and spleen could also be locations where these cysts could also be located. 03:38 Intracerebral hemorrhage all because of what? Hypertension. 03:41 What's lacunar infarct mean? It means little blood vessels up in the brain in which they are undergoing infarction. Lacunar infarct. 03:50 The consequence depending as to what part of the brain that little blood vessel is supplying will then determine the clinical manifestation. 03:59 If it's that part of the brain that isn't so important, then maybe perhaps, not so much of symptoms of your patient. 04:05 But what if it was a little blood vessel supplying the vasoganglia? Uh-oh, we have issues with motor, oh, yeah, you see my point? Lacunar infarct could be significant or insignificant in terms of its presentation. 04:18 Let's move on. 04:19 Chronic renal failure that as far as ADPKD insists, it doesn't meant that you're going to renal failure immediately, because a chronic renal failure will take place, but it's a lot later in life. 04:33 Look at what's bolding, slowly expanding cysts and accounts for approximately 10% of cases of CRF. 04:42 And that would be the most common cause of death at some point if chronic renal failure does set in but you do have time to properly manage your patient is my point. 04:52 Cysts in the liver, older patient, genes of what you're looking for. 04:55 Hypertension will set you, will give you a clue and look for issues within the brain. 05:02 Other associations, now, make sure you understand this. 05:06 Apart from our hypertension, we talked about Berry Aneurysm. 05:10 It could be Sigmoid Diverticulosis, where are you? Left lower quadrant. 05:15 How is that patient going to present? Painless rectal bleeding. 05:19 Hematuria, MVP, what does that mean? In cardiology, we talked about midsystolic click. 05:26 And what about that click? You want that click to be closer to S2, so that the murmur in between it is quite small. 05:33 What else? Slight risk for developing RCC. 05:36 Important associations, not seen overtime, but nonetheless, keep this in mind because when you're reading a clinical vignette, they - trust me, whenever these vignettes are being created, let it be in a journal, boards, or whatever it may be, obviously, it's being put in there on purpose so that it can clue you in on a diagnosis. 05:54 Let's continue.
About the Lecture
The lecture Autosomal Dominant Disease by Carlo Raj, MD is from the course Cystic Diseases (Renal Cystic Pathology).
Included Quiz Questions
Which of the following can cause an atypical physical appearance known as the Potter facies?
- Oligohydramnios
- Small size for gestational age
- Large for gestational age
- Polyhydramnios
- DiGeorge syndrome
Which of the following is NOT an associated complication of autosomal recessive polycystic kidney disease?
- Berry aneurysm
- Potter facies
- Chronic kidney disease
- Portal hypertension
- Hepatic fibrosis
Which of the following is LEAST likely to occur as a result of oligohydramnios?
- Cleft palate
- Lung hypoplasia
- Parrot beak nose
- Low set ears
- Death
Which of the following statements about the inheritance of autosomal dominant polycystic kidney disease is CORRECT?
- It is predominantly caused by mutations in PKD1 or PKD2 genes.
- It is most commonly caused by a defect on chromosome 6.
- All the choices provided are correct.
- PKD2 gene defect is on chromosome 16.
- PKD1 gene defect is on chromosome 4.
In autosomal dominant polycystic kidney disease, at what age does end-stage kidney disease most commonly develop?
- More than 50 years
- Neonatal period
- Infancy and early childhood
- 2nd or 3rd decade of life
- 4th or 5th decade of life
Which of the following statements about the epidemiology and prognosis of autosomal dominant polycystic kidney disease is CORRECT?
- It accounts for approximately 10% of all cases of end stage renal disease in adults.
- It accounts for approximately 25% of all cases of cirrhosis in adults.
- It often presents in childhood.
- Portal hypertension-related complications are the most common cause of death in this population.
- Hypertension is present in less than 50% of cases.
Which of the following is NOT commonly associated with autosomal dominant polycystic kidney disease?
- Retroperitoneal fibrosis
- Colonic diverticula
- Cerebral aneurysms
- Pancreatic cysts
- Cardiac valve disease
Author of lecture Autosomal Dominant Disease

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
