Playlist
Show Playlist
Hide Playlist
Aspirin, Clopidogrel, and Abciximab

-
Slides Hematology-Pharmacology.pdf
-
Download Lecture Overview
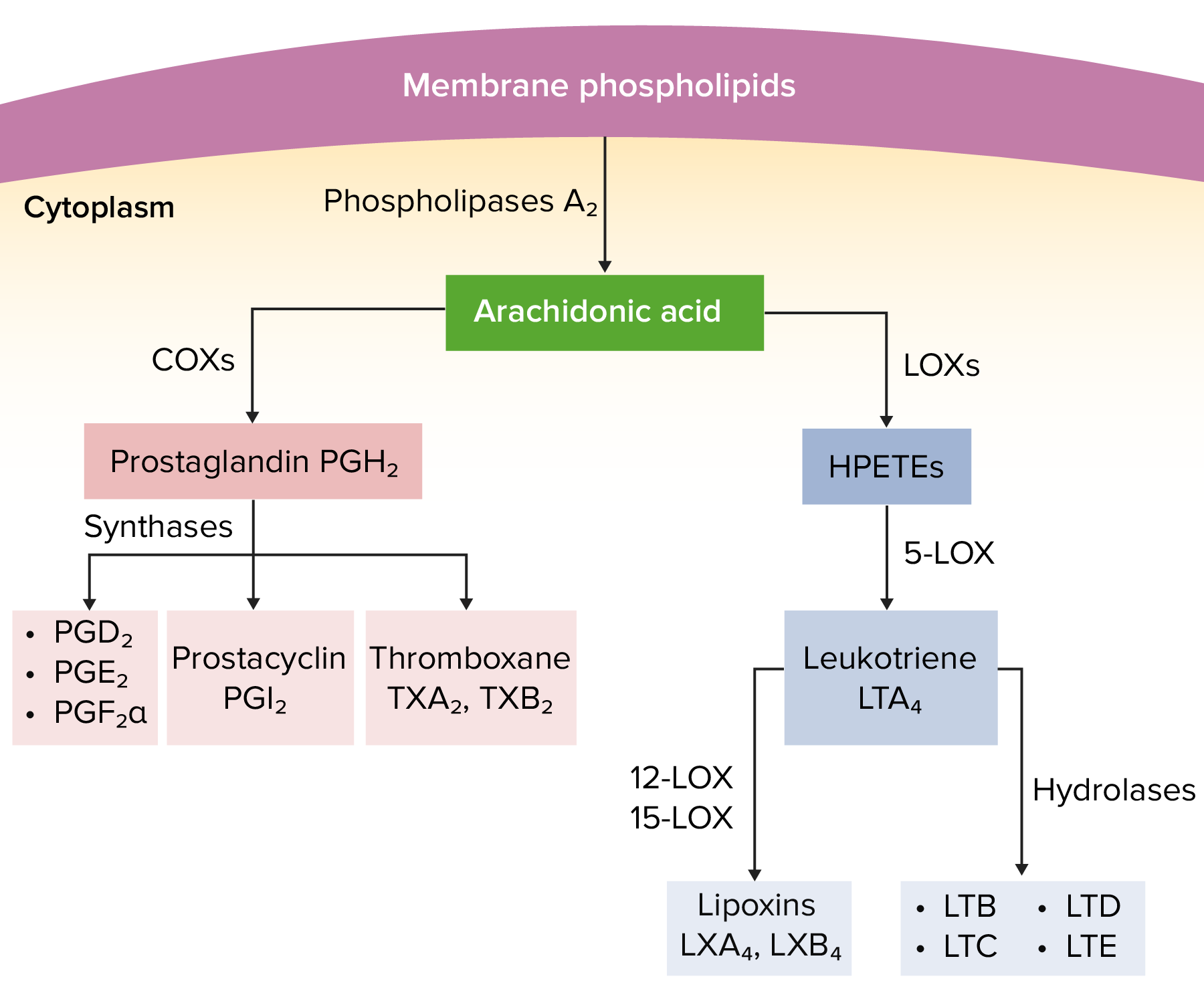
00:01 Aspirin, so we know that it irreversibly inhibits COX pathway both one and two, and so therefore without this, you don't have the thromboxane, guess what you'd lose? Platelet aggregation. 00:16 Bleeding time is the only thing to be affected, and increase in, but no change in PT, PTT, why please? Why? Because we're only dealing with platelets. 00:28 Is that clear? May I ask another important question? Will there be a decrease in platelet count if all that you do is inhibit thromboxane formation, of course not. 00:39 The platelet count will be perfectly normal. 00:42 Clinical use, antipyretics, so for example, patient has fever, analgesia, anti-inflammatory, and antiplatelet. 00:50 Toxicity here, you're thinking about bleeding. 00:53 Now, this is interesting. 00:54 I need you to memorize this. 00:56 In physiology and in a patient that unfortunately may be popping in too many aspirin pills, over the counter, popping these like crazy maybe because they're wishing to take care of a headache and unfortunately, the first thing that may happen for reasons that we're quite unsure of but please memorize that aspirin up in the respiratory center will stimulate it. 01:22 Yes, stimulate it acutely. 01:26 So one of the first things that you're going to find with aspirin toxicity if a patient is taking too many, it actually stimulates the respiratory center which means that the patient has hyperventilation. 01:37 Now, what does that mean to you? On your labs, what are you looking for? An ABG has been done. 01:42 An ABG, what are you going to find in terms of your carbon dioxide? Decrease in carbon dioxide. Welcome to respiratory alkalosis. 01:53 Keep that in mind, very important. 01:55 In addition, they're taking aspirin. 01:58 Who is? A child. 02:00 Maybe the child has, who's this patient? The child, eight years of age, fever, big time. 02:07 Take a look at the tongue, it looks like a peel of a strawberry in a child. 02:12 Fever, strawberry tongue. 02:15 Take a look at the skin of this child. 02:17 It looks like the skin is falling off. 02:20 It's called a desquamating rash. 02:22 Maybe you have lymphadenopathy. 02:24 You put all this together, you should be thinking Kawasaki. 02:26 But with Kawasaki, maybe this child has been taking aspirin. 02:30 Right? It could be. 02:31 Now, I know in clinical practice, we use IVIG granted. 02:35 However, you might be given a situation where such a child is given aspirin. 02:39 You think that child may ever, ever experience a viral infection? Influenza, maybe chicken pox, what have you, and the patient's taking aspirin. 02:51 Now, for reasons that once again are unclear but yet we know is that in that child, a virus plus aspirin may result in death of the liver, highlight, it makes you pay attention to Reye's syndrome and it also has a side effect, Tinnitus. 03:07 It may affect your vestibulocochlear nerve. 03:10 Told you earlier whenever you see the letters GREL, G-R-E-L, what exactly are you doing? Good, you are then inhibiting your P2Y12 receptors. 03:23 You see where it says irreversibly blocking ADP receptors? The name of those receptors are P2Y12 receptors. 03:29 Once you inhibit those receptors and then, what are you doing? You're inhibiting the activation of the platelet. 03:37 If you inhibit the activation of platelet, obviously, I am going to then inhibit aggregation. 03:42 Welcome to Clopidogrel, Prasugrel, Ticagrelor, or Ticlopidine. 03:48 Clinical use once again as an alternative for aspirin. 03:52 So therefore, you're thinking about acute coronary syndrome once again. 03:55 Let it be unstable angina, maybe coronary stenting, and increased incidence of recurrence of thrombotic stroke, a thrombotic stroke. 04:04 Not embolic but thrombotic. 04:05 In other words, maybe a thrombi formation in the middle cerebral artery. 04:10 Those are clinical uses. 04:11 The toxicity especially Ticlopidine, would be neutropenia. 04:16 Look for a patient that has susceptibility to infection. 04:19 Let's take a look at Abciximab here. 04:22 Abciximab is going after what? A glycoprotein IIb/IIIa, picture that for me one more time. 04:29 You have one IIb here and we have another IIb/IIIa here. 04:34 And you have Dr. Roger's ugly face. 04:36 My ugly face is fibrinogen. 04:39 You'll never forget that. 04:41 Welcome to Abciximab. 04:43 Clinical use, as an alternative for aspirin would be acute coronary syndrome. 04:47 It could be part of the regimen of percutaneous coronary angioplasty when you need to go in there and open up and balloon your coronary to make it easier. 04:57 And then, toxicity here may be bleeding and thrombocytopenia.
About the Lecture
The lecture Aspirin, Clopidogrel, and Abciximab by Carlo Raj, MD is from the course Hemostasis: Basic Principles with Carlo Raj.
Included Quiz Questions
Aspirin affects which of the following enzymes?
- Cyclooxygenase 1 and cyclooxygenase 2
- Lipoprotein lipase
- NADPH oxidase
- Nitric oxide synthase
- Hydrolase
Which of the following is LEAST likely to be associated with aspirin toxicity in adults?
- Reye syndrome
- Excessive bleeding
- Stomach ulcers
- Hyperventilation
- Tinnitus
Which of the following best defines Reye syndrome?
- Rare aspirin-associated syndrome of rapidly progressive encephalopathy with hepatic dysfunction in children
- Rare aspirin-associated syndrome of rapidly progressive encephalopathy with hepatic dysfunction in adults
- Common aspirin-associated syndrome of rapidly progressive encephalopathy with hepatic dysfunction in children
- Common aspirin-associated syndrome of rapidly progressive encephalopathy with hepatic dysfunction in adults
- Common aspirin-associated syndrome of rapidly progressive encephalopathy with hepatic dysfunction in both children and adults
Author of lecture Aspirin, Clopidogrel, and Abciximab

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
