Playlist
Show Playlist
Hide Playlist
Arthritis: Treatment




-
Slides Arthritis ChronicCare.pdf
-
Download Lecture Overview
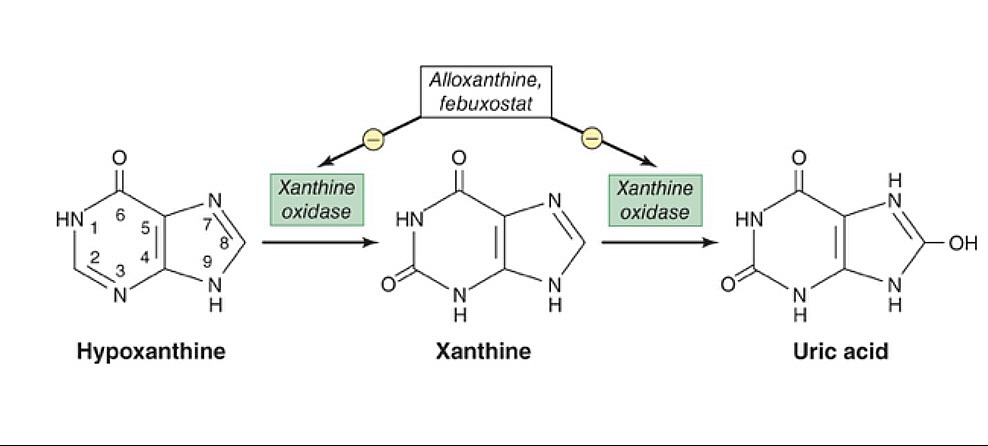
00:01 Okay. Osteoarthritis is the most common kind of arthritis. 00:04 Let’s talk about treatment. 00:06 Once again, I’ve hit on the same theme. 00:08 Acetaminophen is generally less effective than NSAIDs moderately, but it's a lot safer. 00:13 That’s why it’s usually considered first-line. 00:16 It's amazing that tramadol or opiates are recommended or used for osteoarthritis because even in clinical research they really aren't very effective at all. 00:26 Sometimes not much more than placebo and less so than NSAIDs. 00:30 So, therefore, they don't have a strong role among patients with osteoarthritis. 00:35 But corticosteroid injections can help. 00:38 And this is the kind of ladder. 00:39 Start with acetaminophen and NSAIDs. 00:42 NSAIDs try to – I try to keep them – I’ll keep them high dose, but limit for the most severe types of pain. 00:48 If that fails, I’ll actually send the patient directly in for a corticosteroid injection. 00:54 Typically, it's going to be knees. 00:56 Sometimes, it’s going to be shoulder or hip. 00:59 But those injections are relatively safe. 01:01 There's very few systemic side effects. 01:04 And they can generally go for injections four times per year. 01:08 But say they're doing worse and the injections didn’t work anymore, if they’re getting only three or four weeks of improvement, then they need another injection. 01:18 We can’t do that many injections. 01:20 We can’t do 12 injections per year obviously. 01:23 Unfortunately, that’s the time to think about surgery. 01:25 So, when other treatments fail and the symptoms are limiting function, so that's the other key criteria, I think, for joint replacement would be not only is it painful, but it's painful and it limits what I'm able to normally do, think about surgery. 01:43 How about rheumatoid arthritis? How do we go about managing that? So, the treatment really is different and it’s that early initiation of DMARDs (or disease-modifying anti-rheumatalogic drugs), that's key. 01:56 We often start with methotrexate and hydroxychloroquine. 01:59 That's still effective. 02:00 Even though they are older agents, those are effective for a lot of patients with rheumatoid arthritis. 02:07 And with biologic therapies, there's a lot of different options out there. 02:13 Certainly, you want to initiate them sooner rather than later. 02:16 You don't want to let them linger on just methotrexate or hydroxychloroquine when they're progressing in terms of their disease, but choosing between them can be very complicated. 02:25 Their side effects can be complicated and, therefore, it's best left to the rheumatologist. 02:29 But don't forget, these patients are still going to have acute flares. 02:33 There's evidence that both NSAIDs and corticosteroids can be effective. 02:36 They work about equally well. 02:38 For most patients, the side effects of NSAIDs, while prominent, are less than that of corticosteroids. 02:44 So, try to stick to those. 02:47 How about gout? We haven't talked about that as much. 02:50 So, gout starts with lifestyle, avoiding foods and drinks associated with higher rates of uric acid and more gout. 03:00 Allopurinol or febuxostat, they're both effective for reducing the concentration of uric acid and, subsequently, the risk of flares of gout. 03:12 Colchicine is a second line drug. 03:14 And during flares itself, that’s not the time to initiate uric acid reduction therapy. 03:20 Treat till the exacerbation terminates with either NSAIDs or corticosteroids. 03:27 Again, they work about equally well. 03:29 So, for most patients, NSAIDs are a better choice. 03:32 So, that was a brief review of arthritis and, hopefully, you got a sense of avoiding the overuse of routine rheumatologic tests where there's going to be a lot of false positives that throw you off the track, but do use x-rays early in cases of osteoarthritis. 03:51 We talked about the ladder of treatment for osteoarthritis and the early initiation of DMARD therapy for rheumatoid arthritis. 03:58 Thanks very much.
About the Lecture
The lecture Arthritis: Treatment by Charles Vega, MD is from the course Chronic Care.
Included Quiz Questions
Which of the following is most characteristic of osteoarthritis?
- Asymmetric distribution
- Positive serology
- No symptoms in the mornings
- Normal X-rays in late disease
When is the most appropriate time for surgical joint replacement in the treatment of osteoarthritis?
- When conservative therapies have failed to provide adequate pain relief
- Before corticosteroid injections are required for pain relief
- Upon diagnosis
- Early on during the course of disease
- When rheumatoid arthritis coexists
During a flare of gout, what are the preferred treatment options?
- NSAIDs or corticosteroids
- Initiate uric acid reduction therapy immediately during the flare.
- Use of opioids for pain management during the flare.
- Employ dietary modifications without medications during the flare.
- Treating the flare with colchicine as the first choice of medication.
Which of the following medications is generally recommended as the initial pharmacotherapy for active rheumatoid arthritis?
- Methotrexate
- Prednisone
- Acetaminophen
- Indomethacin
- Hydroxychloroquine
Author of lecture Arthritis: Treatment

Charles Vega, MD
Customer reviews
4,3 of 5 stars
| 5 Stars |
|
2 |
| 4 Stars |
|
0 |
| 3 Stars |
|
1 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
3 customer reviews without text
3 user review without text
