Playlist
Show Playlist
Hide Playlist
Aortic Dissection: Signs, Symptoms, Diagnosis and Treatment

-
Slides VascularDisease CardiovascularPathology.pdf
-
Download Lecture Overview
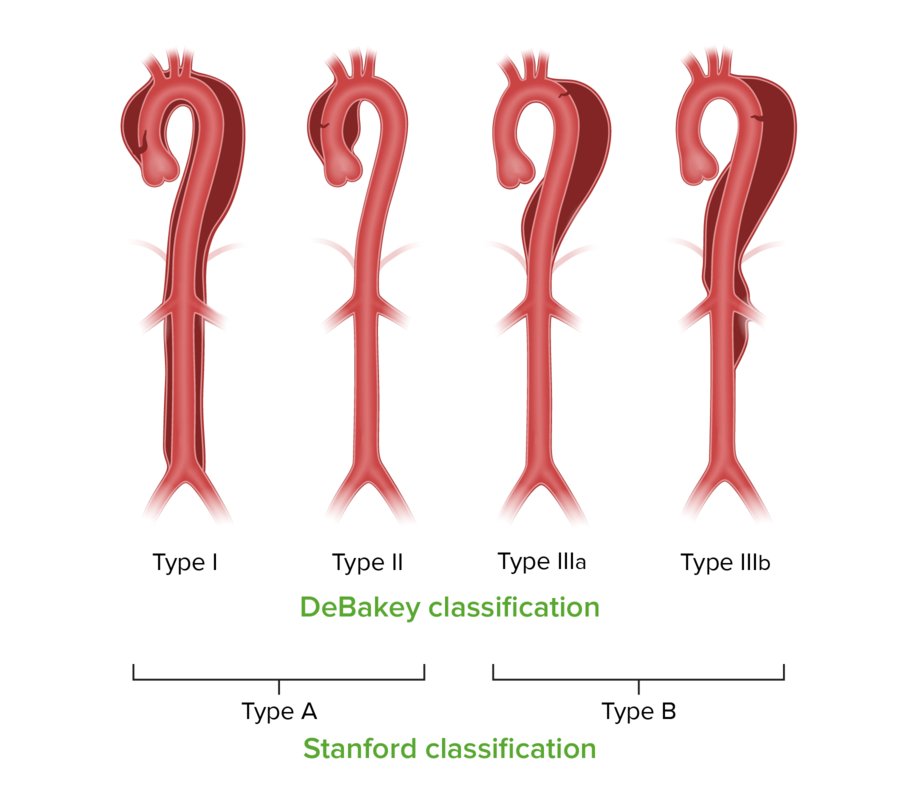
00:00 What about the signs and symptoms? Chest pain, tearing, radiating to the back. Doc, well this thing hurts on a scale of 1 out of 10, 10 being the worst pain the patient has ever experienced, it is a 10, radiating to the back, severity and intensity. Sudden onset because of dissection. What about the patient’s unequal blood pressure where? I just told you the robbing the blood because of the dissection it is removing the blood. 00:32 Not removing the blood, you are losing the blood literally. Unequal blood pressure in both arms due to dissection, obstruction of branches of the aorta. You have issues there because of dissection. Look for that, please. 00:45 The most rapid means of providing sufficient detail to proceed directly to the operating room is with the trans esophageal echocardiogram. 00:52 It's recommended for hemodynamically unstable patients, but requires procedural sedation, which may have adverse effects. 00:58 A TEE is fast, minimally invasive, and can be used in unstable patients or those with renal insufficiency or contrast allergy. Patients who are stable enough to go to a CT scanner from the emergency department more commonly get a CT for diagnosis of aortic dissection. 01:13 This requires contrast injection the diagnosis of aortic dissection by CT requires identification of two distinct lumens, and the intimo flap may or may not be seen. 01:23 A magnetic resonance angiogram is another imaging test that may be used in hemodynamically stable patients. 01:28 Diagnosis made by CT and on this particular CT you will notice right in the middle where there is a tear of your aorta resulting in blood quickly leaking out and resulting in all kinds of issues including that unequal blood pressure between the arms to the point where maybe there is the pericardial cavity effusion or in other words rapidly there might be a tamponade and that is exactly what the middle portion of the CT is then showing you. Diagnosis. Control of blood pressure. Usually, ICU, IV nitropusside and perhaps you are thinking about esmolol or other IV beta blockers because you are trying to control that bleeding that is now taking place quite a bit. You don’t want that cardiac output to be quite high because that is then going to then contribute to the blood being lost through the dissection. That must be understood. You want to relax the heart so that you have control of the dissection. Medical management. The only one that I will be point out here to you will be Stanford type A. 02:41 A is ascending type of dissection. It is persisitent pain, persistent dissection which then requires immediate surgery. 02:50 A, ascending. B, distal, by the thoracic and descending aorta.
About the Lecture
The lecture Aortic Dissection: Signs, Symptoms, Diagnosis and Treatment by Carlo Raj, MD is from the course Arrhythmias: Basic Principles with Carlo Raj.
Included Quiz Questions
What is the rationale behind the Stanford classification of aortic dissection?
- The classification guides treatment based on the area of the aorta involved in the dissection.
- The classification is based on the anatomic location of the initial tear.
- Type A presents acutely, while type B presents chronically.
- Type A involves a true lumen, and type B involves a false lumen.
- They have different etiologies.
Which imaging modality is most commonly used to diagnose an aortic dissection in a hemodynamically STABLE patient?
- CT chest and abdomen with IV contrast
- Aortography
- Transesophageal echocardiogram (TEE)
- Chest x-ray
- Transthoracic echocardiogram (TTE)
In a patient presenting with Stanford type A aortic dissection, what is the mainstay of management?
- Emergency surgical correction
- IV esmolol
- IV digoxin
- IV morphine
- IV nitroprusside
Author of lecture Aortic Dissection: Signs, Symptoms, Diagnosis and Treatment

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
If you want your education to elevate to another level, to be ready for rotations, and to be the best medical professional you want to be....listen to DR. Raj!
