Playlist
Show Playlist
Hide Playlist
Aortic Aneurysm: Diagnosis

-
Slides 04 VascularMedicine advanced.pdf
-
Reference List Vascular Medicine.pdf
-
Download Lecture Overview
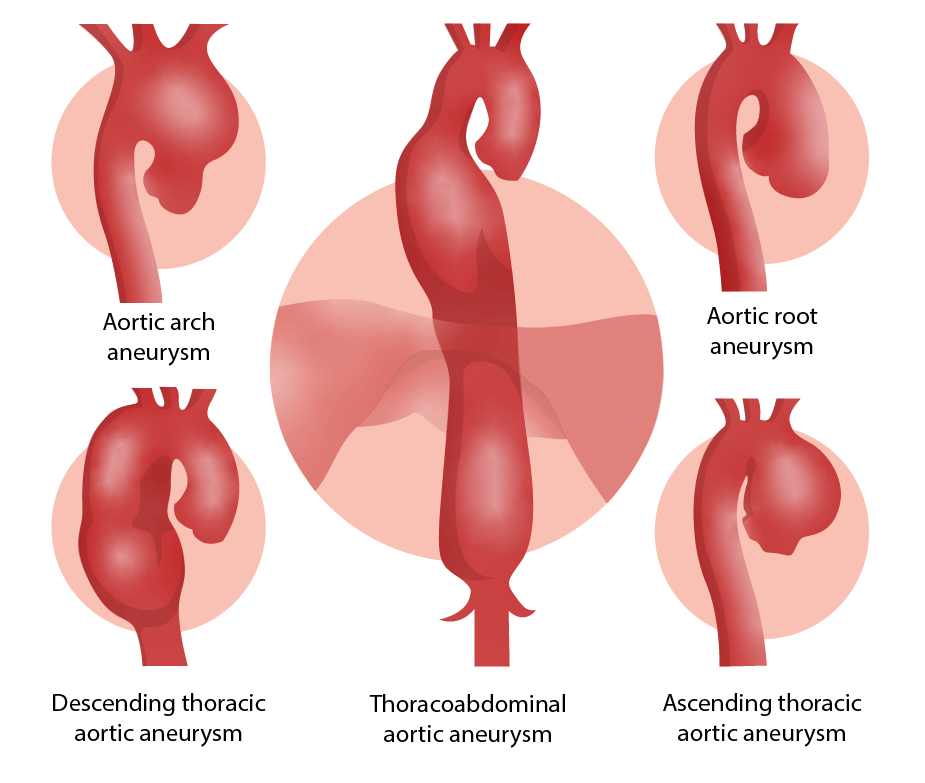
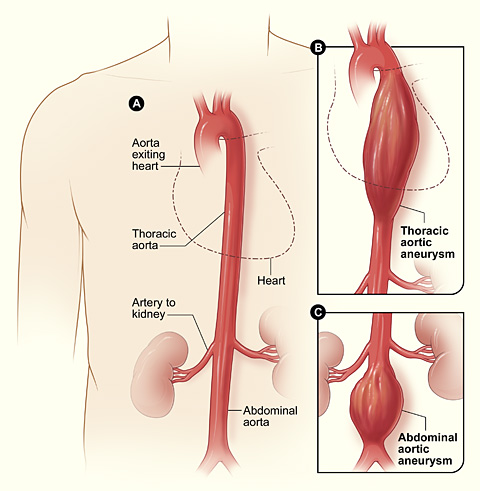
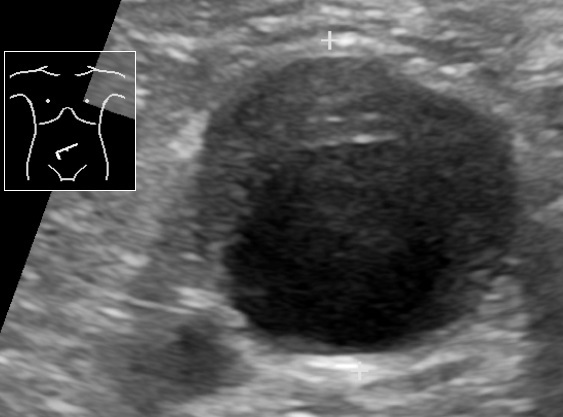
00:00 The diagnosis, again remember that most of them are below the renal artery. 00:07 Sometimes they can be found on physical exam, with a careful abdominal physical exam you may feel a pulsating mass enlargement of the aorta although that is often not seen and the best way is usually to do some form of imaging. 00:28 Sometimes, if the patient is quite thin, you can estimate, you can feel the aorta by pressing deep into the abdomen. 00:36 You can estimate how many centimetres wide it is and feel if it is in fact widened. 00:43 But generally the best technique is using some non-invasive technique to image the aneurysm. 00:51 Aneurysms may be calcified. 00:53 And as I mentioned the potentially fatal complication is when the aneurysm breaks and blood hemorrhages out into the abdominal cavity or the chest cavity depending upon where the aneurysm is located. 01:07 Again the diagnosis is made with either an ultrasound examination of the abdomen or the chest or with an echocardiogram looking at the heart and ascending aorta or with CT scans or MRI imaging and the figure that you see here shows an ascending aortic aneurysm labelled ‘A’, big wide dilated aorta. 01:33 This is an ascending aortic thoracic aneurysm. 01:40 Now the diagnosis again is almost always confirmed even if you suspect it on your physical exam with an ultrasound examination, with echocardiography for thoracic aneurysms, and for abdominal aneurysms usually a CT scan or an MRI. 01:57 In the US usually it's a CT scan that is simpler, takes less time, and gives a very good picture of the aorta and shows you how wide the aneurysm is and often patients who have an aortic abdominal aneurysm are followed every year with a CT scan to see if it is enlarging. 02:15 And when it gets up around 5.5 cm or a little bit more those patients are referred either for surgery or for angioplasty because the risk for rupture is increases at that size. 02:29 Therapy, well if you see an aortic aneurysm starting, then of course one attempts to reduce all of the atherosclerotic risk factors. 02:39 Smoking cessation is very important and particularly in very elderly patients where repair is unlikely to improve the life expectancy, it is important to do as much as you can to control blood pressure, to reduce lipids with statin drugs for example, and of course to get patients away from smoking. 03:02 We often try and hold the blood pressure down, even lower than the usual level, to put less stress on the aneurysm and to decrease its chance of enlarging. 03:14 One can repair them as we have mentioned before either with angioplasty, with stents, or with a surgical repair where the section of the aorta is removed or opened and a graft issewn in, usually are made from Dacron, an artificial plastic substance so that then there is no risk of rupture because the aneurysm is no longer in the circulation.
About the Lecture
The lecture Aortic Aneurysm: Diagnosis by Joseph Alpert, MD is from the course Arterial Diseases.
Included Quiz Questions
Which of the following statements regarding abdominal aortic aneurysms is INACCURATE?
- A diameter of 2.5 cm confirms the diagnosis.
- The majority are infrarenal.
- A pulsating mass may be noticed on abdominal examination.
- They may be calcified.
- They may rupture.
Which of the following imaging techniques most accurately defines an abdominal aortic aneurysm?
- Contrast-enhanced computer tomography scan
- Electrocardiography
- X-ray
- Non-contrast computer tomography scan
- Ultrasonography
What is the size threshold for elective repair of an abdominal aortic aneurysm in asymptomatic patients with a good surgical risk?
- 5.5 cm
- 3 cm
- 3.5 cm
- 4.5 cm
- 4 cm
Author of lecture Aortic Aneurysm: Diagnosis

Joseph Alpert, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
