Playlist
Show Playlist
Hide Playlist
Antidepressants

-
Slides Antidepressants Psychiatry.pdf
-
Download Lecture Overview
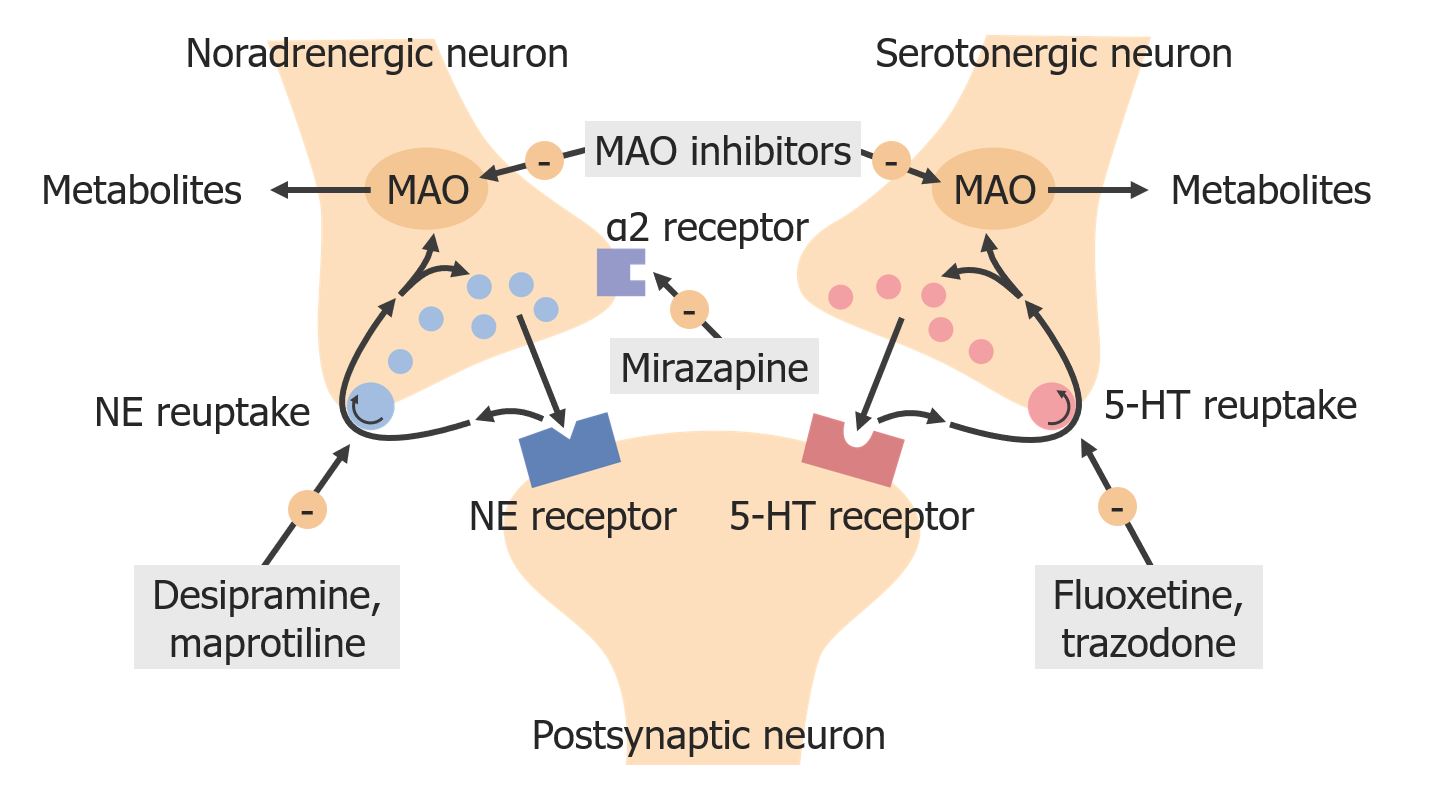
00:01 Treatment with antidepressants is a very important topic. 00:05 So let’s look at some of the highlights here. 00:07 Some of the most commonly prescribed antidepressant medications include the tricyclics, MAOIs, SSRIs, and there are also atypical antidepressants. 00:18 So we’ll take a moment to review the highlights of each. 00:21 When it comes to tricyclic antidepressants, there are a lot of different examples as you can see; imipramine, amitriptyline, the list goes on and on. 00:30 So the mechanism of action here is that these medications will actually block the reuptake of both noradrenaline and serotonin. 00:39 Some of the major uses include depression, enuresis, OCD, and fibromyalgia. 00:45 So as you can see, these medicines can actually be used for things other than depression, although they are labeled as antidepressants. 00:53 Some side effects are anticholinergic problems like urinary retention. 00:58 And also, you get some alpha-adrenergic side effects, including sedation. 01:03 So the toxic effects can be fatal when it comes to TCAs. 01:09 So you’re going to be very careful to not use these medications in the very elderly patient. 01:16 And also, you won’t use it in somebody with suicidal ideation or a plan because overdose on only a small amount of these medications can actually be highly lethal. 01:26 So it causes the three Cs: convulsions, coma, and cardiotoxicity. 01:33 The mechanism of action again, it’s inhibiting noradrenaline and serotonin, increasing their amounts in the synapse. 01:40 Now, here’s a pearl of information. 01:42 These are rarely first line agents. 01:44 And again, that’s due to their cardiotoxicity. 01:48 With TCAs, you always want to start a patient on a very low dose. 01:54 They can get anticholinergic side effects, and this may lead to them not being compliant with the medication. 02:01 Now, if you’re a visual learner, we listed out the side effects here again. 02:06 So sedation, hypotension, tachycardia, arrhythmias, dry mouth, and constipation, urinary retention, blurry vision, weight gain, and again, that ever most important side effect of lethality, something to keep in mind. 02:21 The reason that there are potentially so many side effects with tricyclic antidepressants is that as their name indicates, they’re tricyclics. 02:31 So they work at a number of receptors. 02:33 They have antihistamine potential, they have antiadrenergic potential, as well as antimuscarinic properties. 02:41 So they really lack specificity, and therefore, you can get a lot of side effects. 02:45 Let’s move on now to talk about the MAOIs. 02:48 These are monoamine oxidase inhibitors. 02:51 So here are some drug examples: phenelzine, tranylcypromine, for example. 02:56 The mechanism of action is to decrease MAO activity resulting in a decrease in amine degradation, and therefore, increase levels of amine neurotransmitters. 03:09 There are a lot of different uses for this medication, and very importantly, MAOIs, are used for atypical depression; something to keep in mind for your exam. 03:18 They’re also very useful in the treatment resistant, patient with depression. 03:23 Some of the side effects, very important to know is the hypertensive crisis, and also, overexcitation, CNS stimulation. 03:33 So if you’re a visual learner, you can check out this graph, depicting the mechanism of action for MAOIs. 03:41 And the problem is that these really prevent inactivation of biogenic amines. 03:46 One really important one to note is tyramine. 03:50 So therefore, people can actually get an overload of tyramine in their symptoms. 03:56 And the link between MAOIs and tyramine is very important to keep in mind for your exam. 04:02 Note again that MAOIs are useful for refractory depression, but they’re again, not first line because of safety and tolerability. 04:12 The side effects include orthostatic hypotension, drowsiness, weight gain, sexual dysfunction, dry mouth, and sleep dysfunction. 04:22 Now, the hypertensive crisis is a potential side effect of MAOIs, and this can be potentially deadly. 04:31 And again, this is where that link between tyramine and MAOIs comes into play. 04:36 So the hypertensive crisis risk elevates when people who are taking this medication eat foods that are rich in tyramine. 04:44 They end up with an overload in their system. 04:47 And so a lot of patients won’t tolerate this medicine because they hardly want to eliminate from their diet their favorite foods including wine, cheese, cured meats, chicken liver, et cetera. 05:00 The hypertensive crisis comes from tyramine, which is found in these favorite foods. 05:05 And MAOs, monoamine oxidase, would usually degrade the tyramine. 05:11 But because it’s being inhibited by this medication, again, people who are eating tyramine reach foods end up with an overload and a hypertensive crisis. 05:21 There’s also another potential drug-drug interaction for patients who take MAOIs. 05:27 If they’re on any other compound that increases serotonin in their systems, such as an SSRI or an SNRI, then these patients are going to be at risk for the serotonin syndrome, and you treat serotonin syndrome by of course discontinuing the offending agents. 05:46 And you can also use cyproheptadine as an antidote. 05:51 Let’s talk now about SSRIs. 05:53 Let’s talk now about SSRIs. 05:55 These are very commonly prescribed medications and really important to know about for your exam and clinical practice. 06:01 So, SSRIs decrease the reuptake of serotonin, thereby increasing the neurochemical in the synapse. 06:09 And SSRIs can be used for whole host of things, not only depression, but they can also be used for anxiety disorders, binge eating disorders, panic. 06:19 The side effects are actually quite mild with SSRIs. 06:22 This makes them a very commonly prescribed medication. 06:26 There can be weight gain, however, and QTC prolongation on the EKG. 06:31 There can sometimes be GI distress, and also sexual dysfunction, which will lead some patients to discontinue the medication. 06:39 Again, if a patient is on too much of this medication, or it’s overlapping with another medicine such as an MAOI, they’re going to be at risk for serotonin syndrome, so too much serotonin in their system. 06:54 And people can also get something called an SSRI discontinuation syndrome. 06:59 This occurs when somebody has been on a higher dose of SSRI, and then abruptly stops the medication. 07:05 Here’s a visual graph of how serotonin is being increased by use of SSRIs. 07:12 And note that SSRIs really have similar efficacy. 07:15 You saw that there are a lot of different choices you can pick from. 07:19 Well, when you’re choosing the right medication for a patient, you’re really going to be thinking about the side effects profile, and also cost. 07:26 So there are some distinct advantages for using an SSRI over other medications. 07:31 There’s a low incidence of side effects, there are no food restrictions, and it’s fairly safe even in overdose, although you do have to monitor a patient for serotonin syndrome in overdose. 07:44 There are a lot of different uses as we talked about before that are even beyond depression uses. 07:51 And then again, a list of some of the side effects that we talked about before, noting that in addition to sexual dysfunction and GI disturbance, some patients can have trouble sleeping or get a headache. 08:02 They may have weight changes on the medication as well. 08:07 When a patient is having a sexual side effect from an SSRI, it can be very dissatisfying, obviously, to their lives. 08:14 And there’s a way to treat that. 08:15 So of course, you could consider reducing the dose of the SSRI or switching to another agent. 08:21 But let’s say you have a patient who’s been severely depressed for a long time and they’re doing really well on their SSRI. 08:27 Let’s say they’re taking fluoxetine and their depression has really lifted and they’re feeling great and they don’t want to change to a different medicine because they of course don’t want their depressive symptoms to return. 08:38 Well, you have other options. 08:39 So, two antidotes to the side effects that cause sexual dysfunction in SSRIs are things like bupropion and also mirtazapine. 08:48 They tend to reverse that sexual dysfunction. 08:51 Now, let’s look at another class of antidepressants, the SNRIs. 08:56 There are a couple of examples listed here, and the mechanism here is that serotonin and noradrenaline, and sometimes dopamine are being increased in a synaptic cleft. 09:06 There are a lot of difference uses for the SNRIs, including diabetic peripheral neuropathy. 09:12 So these medicines have really great anti-pain properties, something to keep in mind for your exam. 09:18 And the side effects are notable for hypertension. 09:21 That’s something that might come up on your exam. 09:23 It can also cause sedation and nausea. 09:26 Here’s another visual list of the side effects: possibly, sexual disturbance again and GI upset, headache, and keeping in mind that hypertension can occur and so can the serotonin syndrome, especially when this medicine is mixed with others like in SSRI or in MAOI. 09:46 So let’s talk about withdrawal from SNRIs because this is actually pretty important as well. 09:51 There is a potential withdrawal syndrome, and it can be seen after only one or three missed doses. 09:56 So, a patient taking an antidepressant who missed their dose or two and starts complaining of a feeling like they’re getting electrical shocks or zaps in their brain, that’s probably a patient who’s taking an SNRI and they’re going through withdrawal. 10:11 There are also atypical antidepressants. 10:14 There is bupropion, which is an NDRI, meaning it increases noradrenaline and dopamine. 10:20 And it has a bit of a stimulating effect because of those two chemicals being increased. 10:25 There’s mirtazapine, which is an alpha 2 antagonist that can cause weight gain and sedation. 10:31 And also, trazodone; this inhibits serotonin reuptake, and the major side effect of it is that it causes sedation. 10:38 For this reason, trazodone is actually frequently used as a sleeping aid, and that’s because the side effect of it is, in fact, sleepiness. 10:48 When it comes to atypical antidepressants and trazodone, keep in mind that a negative side effect is priapism. 10:55 So it’s a very prolonged and painful erection in a man. 11:00 So if you hear about that on your boards or in the clinical wards, think about trazodone being the cause.
About the Lecture
The lecture Antidepressants by Helen Farrell, MD is from the course Mood Disorders. It contains the following chapters:
- Antidepressants
- MAOIs
- SSRIs
- SNRIs
- Atypical Antidepressants
Included Quiz Questions
Which of the following drugs acts by blocking the reuptake of noradrenaline and serotonin?
- Amitriptyline
- Fluoxetine
- Clozapine
- Selegiline
- Mirtazipine
Which of the following conditions is not treated with Selegiline?
- Fibromyalgia
- Hypochondriasis
- Treatment resistant cases of depression
- Atypical depression
- Anxiety
Which of the following groups of antidepressants produces hypertensive crisis when taken with tyramine-rich foods?
- Monoamine Oxidase Inhibitors (MAOI)
- Selective serotonin reuptake inhibitors (SSRIs)
- Tricyclic antidepressants (TCA)
- Atypical antidepressants
- Selective norepinephrine reuptake inhibitors (SNRI)
All of the following statements regarding Citalopram are true, EXCEPT:
- Citalopram along with Selegiline can cause severe hypotension
- They increase synaptic serotonin by decreasing the serotonin reuptake pump in the presynaptic neurons
- Its toxicity can produce QTC prolongation on the ECG
- It can also be used for treating OCD and PTSD
- Stopping citalopram abruptly after usage of a high dose can produce SSRI discontinuation syndrome
What medication can relieve sexual dysfunction due to selective serotonin reuptake inhibitors (SSRIs)?
- Mirtazapine
- Fexofenadine
- Cognitive behavioral therapy
- Escitalopram
What neurochemical changes are seen with duloxetine use?
- Increased serotonin and increased noradrenaline
- Increased serotonin and decreased dopamine
- Increased dopamine and decreased noradrenaline
- Decreased serotonin and increased dopamine
- Decreased serotonin and increased noradrenaline
Which of the following atypical antidepressants can also be used as a sleeping aid?
- Trazodone
- Desipramine
- Tranylcypromine
- Bupropion
Author of lecture Antidepressants

Helen Farrell, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
