Playlist
Show Playlist
Hide Playlist
Analgesics: Definition – Opiates and Sedatives

-
05 - Opiates and Sedatives.pdf
-
Download Lecture Overview
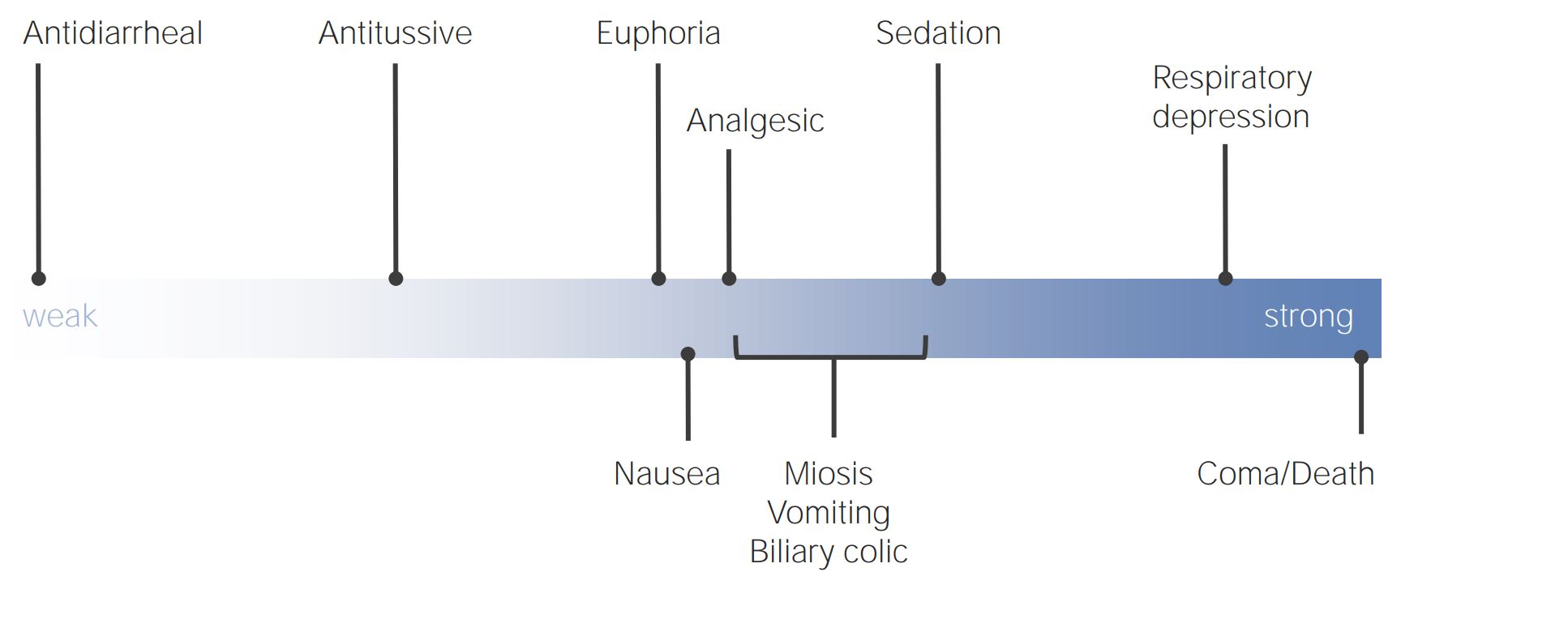
00:00 So what are analgesics? In Wikipedia, analgesic is defined as a painkiller in any number of these groups of drugs used to achieve analgesia, relief from pain. 00:13 It derives from Greek, and the "analgesia" was “without pain.” So an analgesic is something that prevents pain, obviously. 00:25 "Gesia" was "pain." Analgesic drugs act in a variety of ways on the peripheral and central nervous system. Some classes of drugs have no central effect at all. 00:37 Others have little or no peripheral effect. They're distinct from anesthetics, which reversibly eliminate sensations, and they include such drugs as paracetamol (known in North America as acetaminophen or simply as APAP), and the non-steroidal anti-inflammatory NSAIDs, such as salicylates, and opioid drugs such as morphine and opium. 01:07 Additionally, other drugs such as antidepressant drugs, anticonvulsant drugs and some anesthetics at sub-anesthetic doses can also cause, can relieve certain kinds of pain. So we've talked about nitrous oxide and Ketamine previously. So in general, in most parts of the world, non-steroidals and salicylates are non-controlled drugs. And opiates are controlled drugs right across the world. There's actually an international convention that controls these drugs. 01:37 Other analgesic drugs are usually provided by prescription only. Again, depending on where you live. Opioids work centrally in the brain and spinal cord to reduce perception of pain. So they work at every level of the central nervous system and the peripheral nervous system. 01:55 They're either derived from naturally occurring alkaloids, opium from opium poppy, and these are opiates, or they're chemically derived and they're called opioids. I'm going to use these words interchangeably, because they mean the same thing in essence, it just is an indication of where they come from. They're similar in structure, although it's interesting, when you look at them chemically, they don't really look very much alike, but they all have one common feature. They have the ability to bind to opioid receptors in the brain and spinal cord, as do enkephalins and endorphins, which are naturally occurring opiates which we produce within our bodies. These are the most effective drugs for relief of acute pain, surgical pain, trauma pain. 02:49 They all create tolerance, and they create tolerance in 100% of us. 02:55 They all create physical dependency, and they create physical dependency in 100% of us. They all have the potential to create addiction. 03:07 All are controlled drugs. But the incidence of addiction is actually quite low in people who use opioids, even though tolerance and dependency are very common. 03:19 They all produce nausea and vomiting, itching, constipation, and funny feelings, emotional feelings, dysphoria we call it, it's hard to describe, just an unpleasant general feeling. They can all cause muscle rigidity, which is something you probably will never see unless you're giving high doses of these drugs during anesthesia. I've certainly seen that and it's very profound. 03:43 They all have respiratory depressant effects, and can cause death from hypoxemia. 03:49 The comous, when you hear about somebody dying from an overdose of opioids, it's nearly always a respiratory arrest, that is the initiating factor, and then the ongoing development of cardiac arrest and death. So there are a huge number of opioids out there. And they vary by potency, duration of action, mode of absorption. Some of them tend to be very short acting and have less profound effect on respiratory depression than others. Others are very slow in onset, have very long actions, methadone being the classic, and don't produce the dysphoria that addicts seek when they seek narcotics. 04:37 So morphine, heroin, meperidine or demerol, was the, or pethidine in most parts of the world actually, codeine, oxycodone, hydromorphone, fentanyl, sufentanil, which is a 1000 times more potent than morphine and is only used by anesthesiologists, alfentanil, remifentanil, which is very short half-life, about a minute and a half, and again, is only by anesthesiologists. 05:01 And they have a very wide range of delivery methods. You can think of almost any entry to the body, you can give an opioid by that entry. So how do we deal with some of the pain issues associated with surgery? One thing we can do is, we can put in an epidural. And I'll speak more about the difference between epidural and spinal in a future lecture. But let's, at this moment, just talk about putting in an epidural, which is placed before surgery. We put a catheter in, and we use a pump like this, not necessarily exactly like this, to inject, usually a combination of local anesthetics and opioids. And this can produce profound pain relief, particularly for patients who've had thoracic surgery, which is very painful, or abdominal surgery, which can also be very painful. For less severe types of pain we often use patient controlled analgesia. And this is an example of a fairly old pump that we used in our hospital. And you can see, the patient is holding something that looks like a nurse call button. 06:07 It's virtually the same. And the patient can deliver narcotics to himself or herself when it's needed. So, they can push the button, they get a dose of narcotic. 06:19 And you must think to yourself, “Well, isn't there a chance you're going to overdose with that?” Well, it's based on a microprocessor, it's based on metabolic and distribution rates for the normally used narcotics. 06:31 And we always have a lockout period built into the system. So, if you push the button multiple times, you will only get one dose of the drug until such time as a lockout period has passed. At which point, another push of the pump will give you another dose. It works really well. It works extremely well and patients like it, because they feel they have some control. 06:55 One of the things I always advise patients using patient controlled analgesia is, don't wait until the pain's bad. 07:01 Don't be stoical. Get on top of it right away, take the drug early, control the pain and pump, push the button whenever the pain is there.
About the Lecture
The lecture Analgesics: Definition – Opiates and Sedatives by Brian Warriner, MD, FRCPC is from the course Anesthesiology: Introduction.
Included Quiz Questions
Which of the following statements about opioids is TRUE?
- They are second-line agents in the management of chronic pain.
- They are the first-line drugs in the management of chronic pain.
- When part of an anesthetic, they provide a major component of the amnesia required for anesthesia.
- They have few side effects and are well tolerated by nearly all patients.
- They can only be administered by mouth
Which of the following statements about analgesic drugs is TRUE?
- Paracetamol, NSAIDs, and opioids are not the only drugs that can relieve pain.
- Analgesic drugs act only on the brain and spinal cord by reducing the perception of pain.
- Analgesic drugs reversibly eliminate sensation.
- Paracetamol, NSAIDs, and opioids may result in tolerance, physical dependency, and addiction.
- Opioids act by increasing the production of enkephalins and endorphins.
Which of the following opioids is the most potent?
- Sufentanil
- Methadone
- Morphine
- Meperidine
- Oxycodone
Which of the following effects is MOST likely caused by a slow-onset, very long-acting opioid, administered at normal doses?
- Tolerance
- Dysphoria
- Diarrhea
- Muscle rigidity
- Addiction
Which of the following statements about opioids is TRUE?
- Upon cessation of opioids, physical withdrawal symptoms may develop.
- Opioids act only on the brain by reducing the perception of pain.
- Muscle rigidity is a relatively common side effect of opioids.
- Respiratory arrest is usually seen with low doses of opioids.
- Opioids are mainly used for chronic pain relief.
Author of lecture Analgesics: Definition – Opiates and Sedatives

Brian Warriner, MD, FRCPC
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
