Playlist
Show Playlist
Hide Playlist
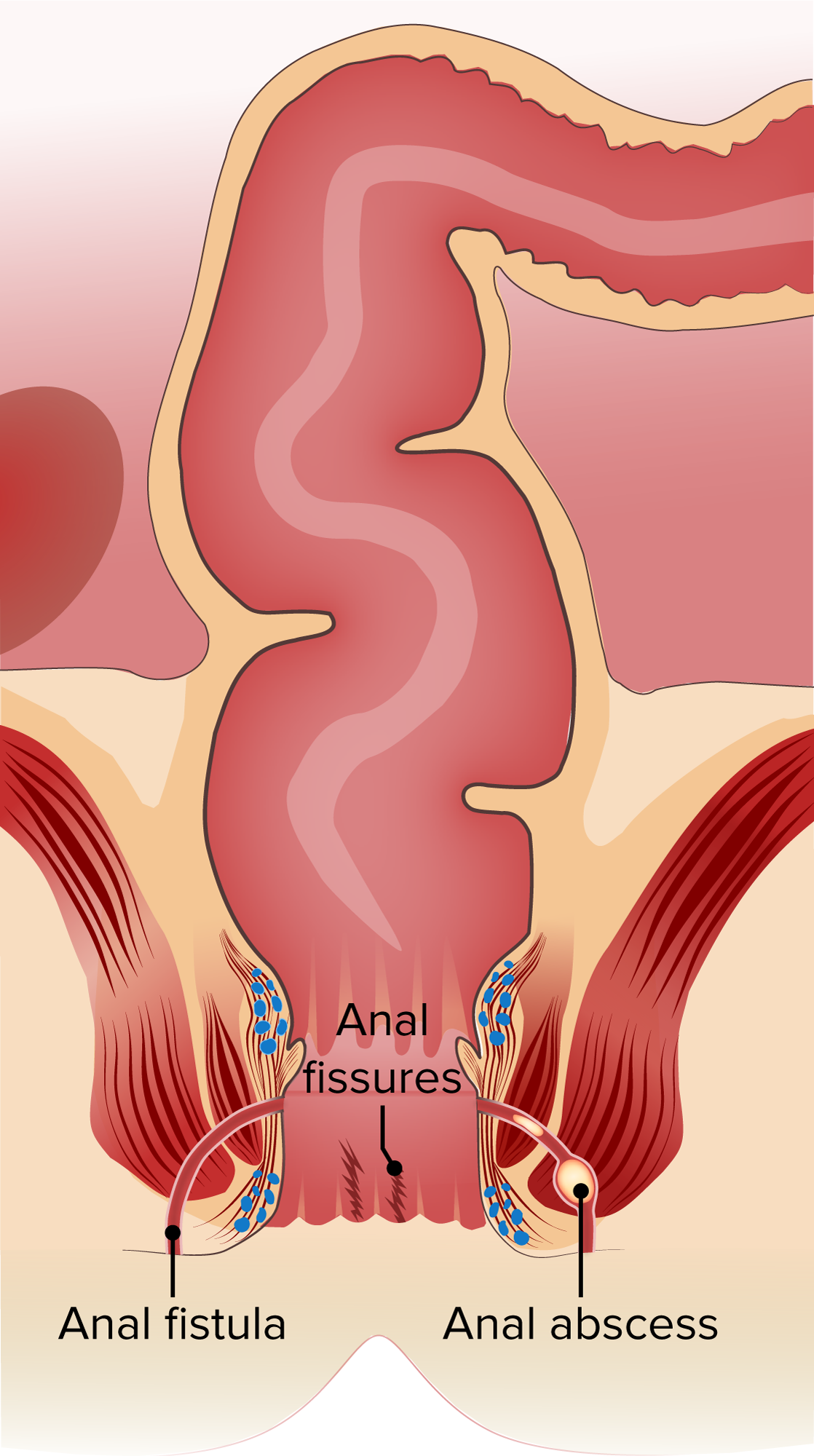
Anal Fissure

-
Slides GIP Anal Fissure.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
00:01 Welcome. With this talk, we're going to discuss a really pleasant topic, anal fissures. 00:08 Anal fissures are just superficial tears of the epithelium right at about the anal canal at or just distal to the dentate line. 00:18 Epidemiology of anal fissures. So, it's most common in young adults. 00:22 Women have this more than men and it's probably related to childbirth more than anything else. 00:29 The incidence overall in the total population is about one in 100 with an 8% lifetime risk. 00:36 Up to 50% of patients with inflammatory bowel disease, specifically, Crohn's disease will have anal fissures. 00:44 If you see it in a child, it's distinctly unusual and that may suggest sexual abuse. 00:50 Other risk factors. So, prior anal fissure is more likely to give you ongoing anal fissures. 00:57 Previous anal surgery with some degree of stenosis of the anal canal due to scarring may make patients at risk for having that epithelial fissural formation. 01:09 In later course, Crohn's disease as we've already mentioned and inflammation in that portion of the bowel, infections, leukemia, squamous cell anal carcinoma are all things that are associated with anal fissures. 01:25 In terms of the pathophysiology, it is fundamentally a mechanical process. 01:30 Forceful dilation, expansion of the anal canal will cause rupturing of the epithelium. 01:37 There is not an infinite capacity for the epithelium to expand. If you dilate that canal, you're going to rip it. 01:44 So, very hard stools, very forceful diarrhea, anal intercourse will all do that. 01:51 Habitual use of cathartics or laxatives by increasing the kind of forceful defecation can also cause this. 02:00 And then, childbirth with third and fourth degree perineal tears. 02:05 So, when you do an episiotomy or when a child is delivered, the vaginal canal may tear. 02:12 But then, if you have a very deep tear, that can involve the anterior segment of the anus. 02:19 Getting to where these occur, so, 90% of them are posterior and these are the shearing forces that occur during defecation. 02:27 Those that are anterior are associated with vaginal deliveries as I've just described. 02:32 If it's not a midline fissure, either anterior or posterior, then, suspect Crohn's disease, infections, anal cancers, or other kind of forceful entry into the anal canal. 02:47 The clinical presentations. So, these are exquisitely painful. 02:51 They're very, very sensitive and the pain will be initiated with defecation and then, will last for hours afterwards. 02:57 Because of the pain, inflammation, etc., there tends to be a spasming of the anus. 03:04 So, patients may describe constipation. And then, because there has been formal laceration, tearing of the epithelium, there will be hematochezia, bright, red blood per rectum. 03:17 The diagnosis, not that hard. This is mostly a physical exam. 03:21 Finding, based on history, if you do suspect there's going to be an anal fissure, don't put in a sigmoidoscope. 03:29 You're just going to have to scrape your patient off the ceiling because of the intense pain. 03:34 You can suspect this based on superficial laceration, some anal mucosa, skin tags that are indicative of hemorrhoids, anal papillae that are hypertrophy and again, this is due to ongoing, increased contraction of the anus. 03:53 If the fissure is not midline or the history's more complicated, then, additional testing may be warranted. 04:00 So, when the pain does subside or when you can administer analgesic, then, you can do anoscopy. 04:07 Biopsy may be indicated to rule out anal carcinoma or other infections. 04:12 In the appropriate setting, you may want to do HIV testing, stool cultures, and then, a more extensive colonoscopy or sigmoidoscopy may be indicated, particularly, in cases where you suspect that there may be inflammatory bowel disease or Crohn's disease. 04:29 How to manage these? Well, there are a number of things. 04:32 And basically, you just don't want them to squeeze so hard and you want the epithelium to heal. 04:36 So, in terms of eliminating some of the reasons for having a forceful defecation, I'll make the stools softer. 04:45 So, the specific laxatives, ingest more fiber. You may want to give topical nitroglycerin or nifedipine and that's to cause some degree of relaxation of the smooth muscle in that area. 05:00 Topical lidocaine is clearly going to be helpful because it's going to be an analgesic. 05:04 You can inject botulinum toxin again to cause relaxation. 05:08 And for intractable anal fissures, may require surgery to actually sew them back up. 05:15 With that, we have reached the end, both literally and figuratively of anal fissures.
About the Lecture
The lecture Anal Fissure by Richard Mitchell, MD, PhD is from the course Small and Large Intestines Disorders.
Included Quiz Questions
What is an individual's lifetime risk for an anal fissure?
- 8%
- 5%
- 15%
- 20%
- 3%
What is NOT a risk factor for anal fissure development?
- Zolpidem use
- Habitual use of cathartics
- Infection
- Crohn disease
- Anal cancer
What is the clinical presentation of anal fissures? Select all that apply.
- Severe onset of anal pain
- Constipation
- Hematochezia
- Hematuria
- Mucus in stool
Author of lecture Anal Fissure

Richard Mitchell, MD, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
