Playlist
Show Playlist
Hide Playlist
Alzheimer's Disease

-
Slides 02 Dementia Neuropathology II.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
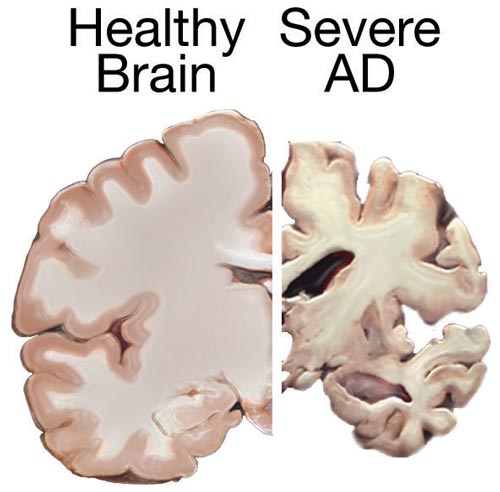
00:02 Let’s talk about Alzheimer’s disease. 00:03 The most common cause of dementia in elderly: slow, relentless, and it’s progressive. 00:10 Oh man, you know when this kicks in, that poor patient. 00:14 And actually, beyond that, what about the surrounding family and friends, huh? Really frustrating. 00:24 Introduce yourself every single day and there’s no guarantee that he or she might remember you the next day. 00:29 Initial symptoms of forgetfulness and memory disturbances. 00:32 Initial. 00:34 Progressive issues with language, and of course, loss of higher function referring to the memory, language skills and such. 00:42 And the total duration from initial symptoms to death, well, it varies but in general, about a decade, and this is something that you want to keep in mind. 00:52 At some point in time, we’ll get into more of your rapid onset, but a decade, in general, from initial onset until death. 01:01 Varies from patient to patient. 01:05 Risk factors: older age, female sex, head trauma, family history, genetics. 01:12 And if you were doing imaging, and this’s a beautiful little schematic. 01:17 Let me show you as to what we’re looking at here. 01:19 On your left is a control or the normal. 01:21 I want you to hone in on the hippocampus. 01:24 And the hippocampus, of course, is responsible for storing your memories. 01:29 And if you compare this control to our patient who has Alzheimer’s disease, well, would you please first take a look at the size of the brain compared to control and the disease on your right? You’ll notice that the size of the brain is extremely, well, much significantly smaller. 01:45 That’s because of your cerebral cortical atrophy. 01:48 In addition, what about the sulci? What does sulci mean? It’s the actual crevice, huh? It’s the crevice between the gyri, and you should know that with anything that is causing cerebral atrophy, that the sulci is going to deepen, deepen, deepen, deepen, deepen. 02:06 So now, it would become a huge gorge because of all that loss of your cortical brain. 02:13 This is not good. 02:14 And if that brain keeps getting smaller, what kind of veins are going to pull on? We had this discussion earlier. 02:21 The veins that it could pull on would be your bridging veins. 02:24 It may result possibly in subdural hematoma. 02:27 You keep going here, please. 02:29 As the brain, the cortex gets smaller and smaller and smaller, then the lateral ventricles look like they’re enlarged. 02:34 Take a look at the disease on the right, and I want you to compare that to the left. 02:39 The lateral ventricles look enlarged. 02:42 That’s interesting. 02:43 That should happen in hydrocephalus. 02:45 Sure. 02:46 Why is the lateral ventricle enlarged here? Well, you’ve lost the brain, the parenchyma, the cortex. 02:52 So therefore, we call this hydrocephalus ex-vacuo. 02:55 And what about the pressure? What pressure? Intracranial pressure. 02:59 Perfectly normal. 03:01 And what about that hippocampus? Look at the control in your left, and you find that hippocampus. 03:07 And on the right, the diseased, Alzheimer’s. 03:10 It’s almost gone. 03:11 It’s almost a cavity now. 03:13 Imagine there being no hippocampus over, let’s say, 8-10 years. 03:18 The memory in this patient, non-existent. 03:21 Beautiful images here of normal on your left and diseased on the right. 03:27 We’re going to start depositing things into the hippocampus and the cortex. 03:32 That is extremely characteristic of Alzheimer’s, aren’t we? So we’ll get into our plaques, and we’ll get into our neurofibrillary tangles. 03:39 Are you ready? Let’s talk about genetic factors. 03:43 This is a huge, huge high yield table. 03:48 So, asterisk this. 03:49 Paste this on your forehead. 03:51 I don’t care what you do. 03:52 Sleep with it. 03:54 This is your table. 03:55 Know everything in it like most of your tables. 03:58 High association with Down’s syndrome. 04:00 I want you to group that and group this together. 04:03 Why? You associate Down’s syndrome. 04:06 APP stands for amyloid precursor protein. 04:09 The topic for this slide is AD, which is Alzheimer’s disease. 04:13 You want to know amyloid precursor protein, you will see why upcoming. 04:17 Look at your chromosome here, 21. 04:19 In other words, you’ve heard of trisomy 21. 04:22 I want you to take a look at the onset of the age. 04:24 In Down’s syndrome, young patient, huh? Less than 35. 04:28 If there is amyloid precursor protein mutation, and I’ll show you why, your patient is a little bit older, but actually, not that old, huh? 45, not that old. 04:38 And early onset with Down’s syndrome, you’re already 35. 04:44 Early onset, it’s already happening. 04:47 With amyloid precursor protein, yes, less than 1%. 04:52 And in terms of percentage of all cases, well, with APP or amyloid precursor protein mutation, less than 0.1. 05:02 But nonetheless, you need to know it. 05:05 Why? Let’s take a look. 05:07 A beautiful picture here that I’m going to walk you through. 05:10 Number one on your left is the amyloid precursor protein. 05:14 And in it, do you see that little green rod? That green rod represents the beta amyloid. 05:21 Look what happens when there is a mutation. 05:24 Holy Moly! Now, the amyloid precursor protein is basically disintegrating. 05:30 And what’s happening is that the beta amyloid is now being detached. 05:34 And look what all of the beta amyloid, those green rods do in illustration number three to your right. 05:40 They’re going to get together, huh? And they’re going to have a grand old time and they form a plaque. 05:45 You see that plaque? In other words, think of it as being a plate. 05:49 This is a plate that is being served in Alzheimer’s disease with beta amyloid. 05:55 That is a huge point. 05:57 These are beta amyloid plaques. 05:59 You could find these mutations. 06:01 This is not a good thing. 06:04 Continue with the table. 06:06 There is something called PS1 mutation. 06:09 This is a chromosome 14 if you can remember it. 06:11 These are early onset. 06:12 Look at this, 28. 06:15 Horrible, horrible. 06:16 By the time your patient is 40, even 35 to 40, I mean, it is severe. 06:22 So, what you can expect in maybe a 70-year-old patient is what you would see in a maybe 35 or 40-year-old patient or even 55, which is still young for Alzheimer’s. 06:30 Keep that in mind. 06:32 Look at this, percentage of early onset, 50%. 06:35 This is a PS1 mutation. 06:37 Percentage of all cases, 1% to 2%. 06:40 That's still very high. 06:41 In my opinion, that’s pretty high, pretty young. 06:44 PS2. 06:46 PS2, here it is. 06:47 I’m not going to talk about this much. 06:49 I’d focus on PS1 if I were you. 06:51 APP, and obviously, Down’s syndrome. 06:53 And you definitely want to know about APOE e4, please. 06:56 Now, APOE e4, you definitely want to know chromosome, everything in this row, 19. 07:02 Age of onset, greater than 60. 07:04 This is the one in which 40% of all cases of Alzheimer’s disease, which you’re going to find issues with. 07:08 It’s called APOE e4. 07:10 In terms of early onset, not applicable here, okay? Not applicable. 07:15 This is the one in which greater than 60, and so therefore, the one that is your classic or traditional type. 07:21 You know the table well. 07:23 Make sure that you pause and make sure you understand amyloid precursor protein and the development of this beta amyloid plaques, and I’ll come right back to it in a few minutes.
About the Lecture
The lecture Alzheimer's Disease by Carlo Raj, MD is from the course Dementia. It contains the following chapters:
- Alzheimer's Disease
- Genetic Factors Linked to AD
Included Quiz Questions
Which of the following is NOT a risk factor for Alzheimer disease?
- Hypertension
- Older age
- Family history
- Female sex
- Head trauma
Which of the following is a typical pathological feature in the brain of a patient with Alzheimer disease?
- Shrinkage of hippocampus
- Expansion of hippocampus
- Shrinkage of hypothalamus
- Expansion of hypothalamus
- Shrinkage of the limbic system
What is the most likely cause of intracranial hemorrhage in a patient with Alzheimer disease?
- Rupture of the bridging veins
- Rupture of the middle meningeal artery
- Rupture of the anterior cerebral artery
- Rupture of the posterior cerebral artery
- Increase in the intracranial pressure
Which of the following is correctly paired in the representation of genetics in Alzheimer disease?
- Amyloid precursor protein and chromosome 21
- APOE e4 and chromosome 21
- Amyloid precursor protein and chromosome 14
- PS2 mutation and chromosome 14
- PS1 mutation and chromosome 1
Which of the following is true in the formation of beta-amyloid plaques in the pathogenesis of Alzheimer disease?
- A detachment of beta-amyloid protein from amyloid precursor protein
- Integration of beta-amyloid protein with amyloid precursor protein
- Beta-amyloid plaques that integrate with the APP
- Beta-amyloid plaques that integrate with the APOE e4
- PS2 mutation that leads to the formation of beta-amyloid plaques
Which of the following genetic factors is NOT related to Alzheimer disease?
- Trisomy 18
- APOE e4 mutation
- APP mutation
- PS1 mutation
- PS2 mutation
Author of lecture Alzheimer's Disease

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
HE IS JUST THE BEST TEACHER THAT LECTURIO HAS EVER HAD IN HISTORY
