Playlist
Show Playlist
Hide Playlist
Alzheimer Dementia: Clinical Manifestation and Diagnosis

-
Slides Alzheimer Dementia.pdf
-
Download Lecture Overview
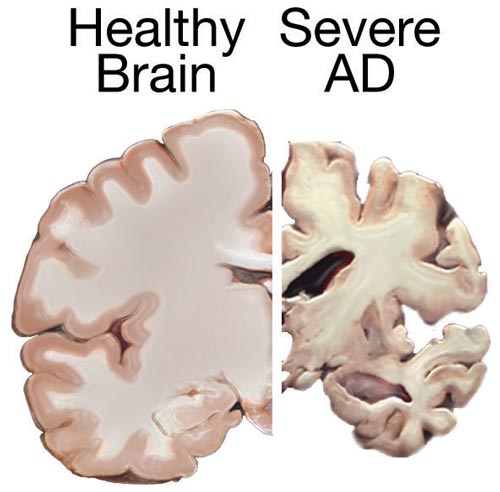
00:00 So let's talk about some of the clinical manifestations that we see with Alzheimer's disease. Alzheimer's is a disorder of memory impairment. This is the most common early symptom of Alzheimer's disease. It's described by patients as an anterograde long-term episodic amnesia. Patients can't remember what you just told them. They knew who they are, they have all their long-term memories, but those new memories that they want to lay down are difficult to do. It is insidious in its onset with slow, gradual progression. It's a degenerative disease, so we see slow gradual progression over time. Rapid onset or episodes of more severe memory loss should prompt in and warn evaluation for alternative etiologies. In the earliest stages of presentation, episodic memory is affected. That's the memory of events occurring at a time or a place, things that we've done recently. We can also see impairment in executive function and judgement. There can be associated behavioral changes and this is more common in advanced stages of the disease. We do look for and can see impairment in other cognitive domains. Again, apraxia, agnosia, aphasia in addition to that early amnesia and this may develop and progress insidiously as well. Patients may develop motor functional impairment. When we think about apraxia or the planning of movements, this appears as difficulty performing purposeful movements; showing how you would brush your teeth or cut a slice of bread or demonstration of how you would do a motor task. We can see behavioral and psychological symptoms, sleep disturbances, apathy or just lack of interest motivation in doing something, social disengagement, or irritability particularly in advanced stages of the disease. 01:52 How do we diagnose Alzheimer's disease? Well, it's a clinical diagnosis. We use our history and physical examination, one to support a diagnosis of Alzheimer's disease and to exclude alternative pathology. A detailed neurologic exam is important. 02:08 Patients with focal neurologic deficits or symptoms and signs that don't fit with typical Alzheimer disease pathology should warrant evaluation of an alternative diagnosis. And then we can use bedside tests to support a diagnosis of Alzheimer's disease and guide us in terms of the severity. And that includes the Mini-Mental Status Exam as well as the Montreal Cognitive Assessment Exam. The Mini-Mental Status Exam is a longstanding used exam, but the MOCA is really more sensitive and specific for stages of Alzheimer's disease and we'll see that used more often in the clinic and with clinical vignettes. So let's talk through both the MMSC (Mini-Mental Status Exam) and the MOCA (Montreal Cognitive Assessment). The MMSC is a test of cognitive function among those in the elderly or other ages. It includes test of orientation, attention, memory, language, and visual spatial skills and so you can see this has been oriented to detect patients who may have Alzheimer's dementia where these domains are primarily affected. Now let's look more specifically at the MMSC. We test each of those important domains of cognitive function and the first is orientation. We look at at year, month, date, as well as location and this is scored out of a total of 5. Next is registration asking the patient to remember 3 items and immediately report them back. 03:37 Patients with advanced dementia can still register items and it's important to evaluate the registration before we test recall. We look at attention and concentration with serial 7s or spelling world backwards or reciting the months of the year forwards and backwards. We're looking to see whether the patient is able to remain on task to maintain their attention and concentration throughout the entirety of that task. 04:05 Fourth is recall. Those 3 words that we ask the patient to remember, can they remember them at 5 minutes, we're looking for short-term memory dysfunction. 04:15 And then lastly, we look at naming and language asking the patient to name and repeat as well as follow commands looking for issues with aphasia in this category and domain. And then the last domain is visual spatial tasks and you can see the inner interweaving boxes, pentagons that are drawn here and the patient is asked to reproduce this image. In terms of scoring, we score the MMSC on a scale of 30. 24-30 indicate no cognitive impairment, 18-23 indicates mild cognitive impairment, and score less than 17 more severe cognitive impairment. Now let's turn to the MOCA, the Montreal Cognitive Assessment which is really the work course in terms of bedside testing of cognitive function. This is a rapid screening instrument for Mild Cognitive Impairment as well as advanced dementia. It consists of 30 questions, takes about 10-12 minutes to complete and can be easily incorporated into a clinic visit or an inpatient hospital examination. What are the domains tested on the MOCA? The first is visual spatial and executive function and a number of tasks evaluate this domain. We look at naming, memory function both immediate and long-term recall, attention is tested. 05:42 Attention and concentration, you can see here with serial 7s as well as repeated word list. And language function. We also look at abstraction, the ability to look at abstract thoughts, delayed recall, remembering things at 5 minutes, and orientation. 06:04 Like the MMSC, this is scored out of a total of 30. Scores between 26 and 30 are normal and patients are considered to have normal cognitive abilities, a score of 19-25 indicates mild cognitive impairment, and scores less than 21 indicate more advanced mild, moderate, or severe dementia. In addition to bedside examination, imaging can be used in the evaluation of these patients. It's not required for a diagnosis but can be supportive in selected cases. In terms of structural imaging like MRI, we really don't see early findings but we can see late findings of an advanced dementia including generalized or focal atrophy, white matter lesions, reduced hippocampal volume or medial temporal lobe atrophy. By the time we're seeing these changes, there is no ability to intervene for the patient and this really is not incorporated into the early diagnosis of Alzheimer's disease or other dementias. 07:02 Increasingly, we see the use of beta-amyloid PET imaging as well as other more advanced nuclear imaging techniques. This uses a tracer that binds to beta-amyloid and lights up areas of deposition of beta-amyloid. We use a qualitative assessment of beta-amyloid plaque density and you can see that here in the images. The red areas are areas of beta-amyloid deposition and we can see those in the frontal lobes as well as the posterior temporal and parietal lobes, areas that we would typically see beta-amyloid deposition in Alzheimer's dementia. And this can be suggestive of early signs and early pathology in patients who have both mild cognitive impairment and more advanced cognitive dysfunction.
About the Lecture
The lecture Alzheimer Dementia: Clinical Manifestation and Diagnosis by Roy Strowd, MD is from the course Alzheimer Dementia.
Included Quiz Questions
What is the most common early symptom of Alzheimer dementia?
- Anterograde long-term episodic amnesia
- Visual hallucinations
- Urinary incontinence
- Behavioral disturbances
- Apraxia
Which of the following are warning signs that should prompt evaluation for causes of dementia other than Alzheimer's disease? (Select all that apply.)
- Rapid onset or episodes
- Focal neurologic deficits
- Severe memory loss
- Impaired concentration
- Difficulty with navigation
The Mini-Mental Status Examination (MMSE) is a useful clinical test in patients with cognitive decline. What does it test?
- Orientation, attention, memory, language, and visual-spatial skills
- Coordination, stability, concentration, and attention
- Dexterity, agility, and wit
- Hearing, light touch and vibration sense, and pain and temperature sense
The Montreal Cognitive Assessment (MoCA) is a test that is extremely useful for patients with cognitive decline. What cognitive functions are tested with the MoCA?
- Visual-spatial/executive functions and memory (short- and long-term recall)
- Oculomotor and vestibular function
- Dorsal column and spinocerebellar tract
- Language, fluency, repetition, and concentration
Author of lecture Alzheimer Dementia: Clinical Manifestation and Diagnosis

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
