Playlist
Show Playlist
Hide Playlist
Acute Dysentery

-
Slides InfectiousDiarrhea InfectiousDiseases.pdf
-
Reference List Infectious Diseases.pdf
-
Download Lecture Overview
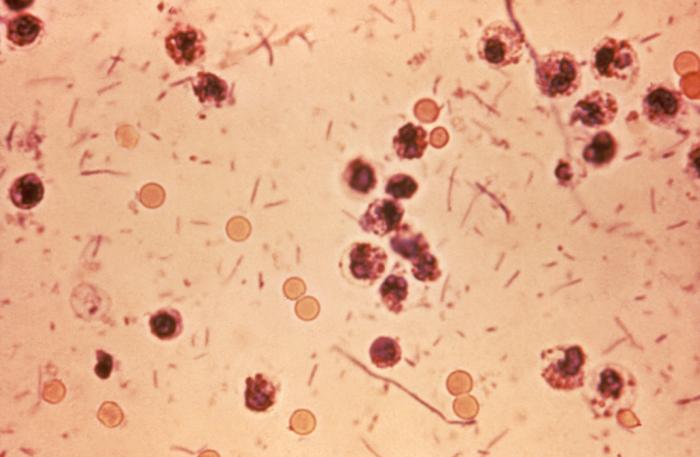
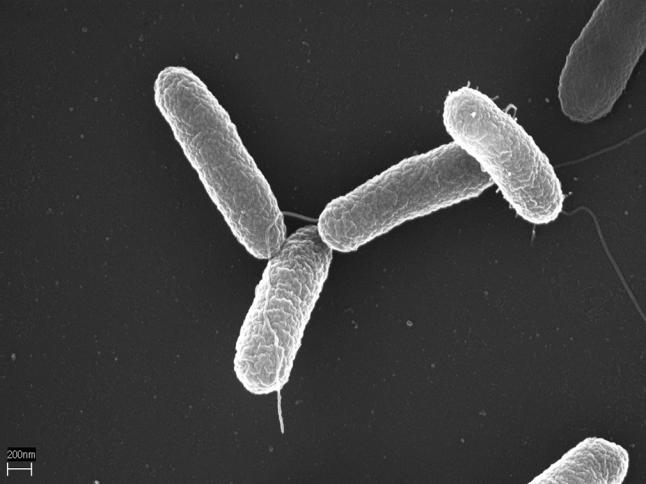
00:00 So now there are other causes of invasive diarrhea such that we call acute dysentery and these patients usually have fever to 38.5 or more and they have stools that are frequent but this is the difference. They are small volume stools with mucus. They are generally unformed and many of these patients have bloody diarrhea. I want to stop here and talk about the small volume diarrhea. So invasive colitis is characterized by maybe frequent stools but small in volume so part of the history that you want to take is "Tell me something about your diarrhea sir" and you want to find out not only how often but the volume of the stool and this is where you also want to ask about tenesmus because if they have the frequent urgency to defecate but without much productivity, that is a big point in favor of a large bowel invasive problem. 01:22 So abdominal cramps and these cramps are going to be localized below the umbilicus, they're going to be in the area of the colon with tenesmus and fecal urgency. Now the causes in the US that are common are Salmonella enteritidis, Campylobacter, Shigella and the uncommon causes would be Aeromonas hydrophila. So when would you think of that organism? Well, the history would tell you that they have had some recent exposure to swimming in fresh water, lake water or maybe brackish water and Yersinia enterocolitica and just a small point about this organism. A lot of these patients will present like they have appendicitis and then the non-cholera Vibrios like for example Vibrio vulnificus or Vibrio parahaemolyticus. In the non-cholera Vibrios, the way to remember those is we're talking about saltwater and these organisms are part of the normal flora of the sea and so if someone has had exposure to food that comes from the sea, a fish, crustaceans and so forth they could get this non-cholera Vibrios invading the colon. Now, dysentery is not that frequent a problem, the outbreaks are pretty infrequent in the United States and a lot of them are caused by enteroinvasive E. coli. 03:17 Let's talk about Salmonella, an important cause of invasive colon disease. There really are 2 species of Salmonella. The first is Salmonella enterica which you usually get from lower animals, it's a zoonosis and in this classification are subspecies numbering 6. Subspecies I (enteritica) contains almost all pathogenic serotypes and here we're talking about Salmonella typhi, the cause of typhoid fever; Salmonella typhimurium and Salmonella choleraesuis and each of these can present in one of 3 clinical patterns, either acute dysentery, septicemia, or enteric fever. 04:14 Now Salmonella typhi is the one that causes most of the enteric fever, the so-called typhoid fever. The other organism is Salmonella bongori which was formally classified among subspecies V. Next, we need to consider Shigella. The Shigella species are Shigella dysenteriae, flexneri, sonnei and boydii. Sonnei is the most common. These are highly contagious organisms. If you ingest as few as 180 organisms and that isn't much if you think about the organisms being maybe 3 microns long and a micron wide. So these are tiny bugs and just ingesting of that few could give you dysentery. Then another cause is enteroinvasive E. coli which causes acute dysentery. This one contains a plasmid which encodes a protein that allows the organism to invade and multiply epithelial cells and also affects actin. It hijacks the actin filament and enables it to spread cell to cell. Another important cause of acute dysentery is Campylobacter jejuni. This probably is the leading bacterial cause of foodborne dysentery and it attaches to intestinal cells and subverts the microtubules in the cell to gain entry and causes rest of the cell cycle, cell swelling and death. So when someone has a history of acute dysentery, they obviously need to see a physician and they need a work-up and the first thing we'll do is do a stool culture and most of these pathogens grow quite well on typical selective agar like MacConkey's agar. That's the most important test in somebody with acute dysentery. Another extremely important test is to examine the stool to see if there are white cells present and I think you can see a number of neutrophils in this particular stool sample and the other thing I hope you've noticed is the red cells so this patient probably did have bloody diarrhea. So we're looking for fecal leukocytes and seeing those tells you we've got an invasive problem. 07:04 There is a more automated test called the fecal lactoferrin and lactoferrin is a glycoprotein that you find in the granules of neutrophils and we can test simply for fecal lactoferrin where it's more difficult to do microscopy on stool and it's more sensitive than doing stool microscopy. 07:32 When we have other diagnostic uncertainties, we may have to employ imaging like a CT scan of the abdomen and occasionally colonoscopy but we wouldn't do colonoscopy on somebody who's got an active inflammation of their colon unless they had persistent or recurrent disease.
About the Lecture
The lecture Acute Dysentery by John Fisher, MD is from the course Gastrointestinal Infections.
Included Quiz Questions
Which of the following is the most common pathogen that results in small-volume diarrhea with hypogastric cramps, fever, elevated fecal lactoferrin, and a Gram-stain of stool which shows curved, Gram-negative bacilli?
- Campylobacter jejuni
- E. coli O157:H7. (HUS)
- Enteroinvasive E. coli
- Salmonella enteritidis
- Shigella sonnei
Which of the following is not a typical symptom of invasive colitis?
- Large volume stools
- Tenesmus
- Lower abdominal cramps
- Mucus in stool
- Bloody stool
Which of the following Shigella subspecies is the most common in the United States?
- Shigella sonnei
- Shigella flexneri
- Shigella dysenteriae
- Shigella boydii
- Shigella typhi
What is the pathogenic mechanism of Enteroinvasive E. Coli (EIEC)?
- The bacteria contain a plasmid which encodes a protein that allows it to invade colonic epithelial cells and multiply within them while also spreading cell to cell via actin filaments.
- The bacteria produce a toxin which creates a pore in the epithelial cell membrane to allow entry of the bacterium body and multiplies within the cell.
- The bacteria contain a plasmid that allows each bacterium to invade the colonic cells one at a time. It is not able to multiply or spread within the cells.
- The bacteria produce a toxin that causes cellular swelling and apoptosis without having to invade the cell themselves.
- The bacteria attach to the intestinal cell walls with their filaments and then spread cell to cell on actin filaments.
Which is the most important diagnostic test for invasive colitis?
- Stool culture on MacConkey's agar
- Stool microscopy for fecal leukocytes
- Fecal lactoferrin
- Computed tomography (CT) scan
- Colonoscopy
Author of lecture Acute Dysentery

John Fisher, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
