At a glance: Clinical reasoning assessment is the systematic quantification of a trainee’s diagnostic workflow, cognitive structures, and decision-making capabilities when managing clinical uncertainty. By utilizing advanced metrics rather than retrospective, checklist-based multiple-choice exams, institutional leaders can objectively measure active synthesis, predict downstream clinical safety, and comprehensively evaluate milestone competencies across diverse medical training cohorts.
Introduction: The Dean’s Mandate in the Clerkship Continuum
Standardizing medical competence across highly fragmented clerkship rotation blocks is one of the most critical operational mandates facing modern undergraduate medical school deans. While traditional retrospective written examinations remain highly valuable for tracking macro-level residency match outcomes, they frequently fail to provide clinical education leaders with granular, step-by-step visibility into how a medical student actively navigates clinical uncertainty in real time. Under programmatic accreditation requirements like LCME Standard 6, institutions must guarantee a structured, comparable clinical curriculum, yet core clerkships routinely suffer from opportunistic, non-standardized patient encounters that obscure a trainee’s true diagnostic acumen.
This assessment gap arrives during an era of unprecedented systemic strain. While the World Health Organization projects a global shortfall of 10–11 million healthcare workers by 2030, the immediate educational consequence is a severe squeeze on faculty teaching hours that directly correlates with rising clinician educator burnout and creates an urgent structural need for independent, residency-ready graduates. In these high-pressure clinical environments, clinical reasoning must extend far beyond initial diagnostic accuracy. Trainees must rapidly master comprehensive management reasoning, therapeutic decision-making, and patient-centered considerations—complex cognitive workflows that are incredibly difficult to evaluate without granular, structured assessment tools.
Compounding this challenge, current graduate medical education literature notes that major international medical governing bodies have yet to establish clear, resident-specific guidelines regarding digital documentation workflows and automated ambient utilities. Consequently, the operational burden of defining, securing, and validating core clinical competency falls squarely upon undergraduate program directors, who must innovate independently to protect institutional reputation, elevate formative assessment quality, and sharpen student diagnostic accuracy.
Mapping “Visible Thinking”: Moving from Passive Checklists to Active Synthesis
Moving learners away from linear digital cases to conversational workflows is essential for externalizing cognitive frameworks and making clinical thinking fully visible to educators. Legacy electronic checklists may encourage recognition-based responses rather than requiring learning to actively generate and justify diagnostic hypotheses. To address this pedagogical shortfall, undergraduate programs require an explicit method to map a student’s dynamic diagnostic timeline as they actively shape competing differentials.
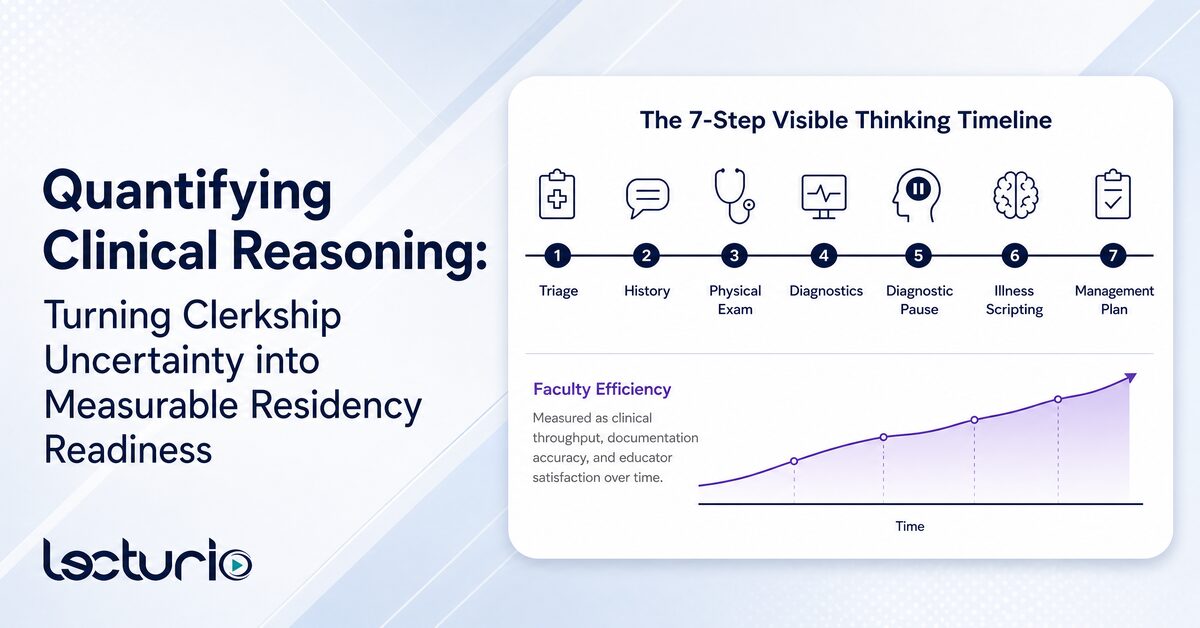
Lecturio’s clinical reasoning platform, Healer, provides an innovative solution by externalizing the learner’s diagnostic workflow across a strict, structured 7-step timeline:
- Triage
- History
- Physical Exam
- Diagnostics
- Diagnostic Pause
- Illness Scripting
- Management Plan
Through specialized product architecture features like the Diagnosis Pad, learners must actively synthesize raw patient findings and draft custom problem representations on the fly. Furthermore, the Diagnostic Pause forces the learner to pause, reflect, and utilize Venn diagrams for visual reasoning, mapping out competing differentials against explicit expert consensus.
Peer-reviewed research underscores the pedagogical superiority of an active approach over traditional semilinear formats. An observational crossover cohort study at Karolinska Institutet found that medical students rated an AI-enhanced social robotic virtual patient platform as significantly more authentic for clinical decision-making than a conventional computer-based platform (P = 0.03). Note: the study design was observational, not randomized. Students also reported perceiving the robotic platform as more beneficial for preparing to manage real patients (P = 0.009), though this reflects self-reported perception, not a measured transfer-of-learning outcome.
By requiring active production over passive consumption, institutions gain a vital layer of objective cognitive metrics that seamlessly complement workplace observations, personalized precision medical education tutoring interactions, clinical simulations, and narrative feedback. Academic leaders looking to see how these reasoning analytics enhance a multi-source assessment framework can Try a case to analyze the structural framework directly.
Overcoming the Feasibility Hurdle: Scaling Script Concordance with Backend AI
Automating advanced formative feedback allows institutions to deploy scalable script concordance evaluation without imposing unsustainable grading burdens on clinical faculty. Traditional clinical assessment methods that successfully probe cognitive networks under conditions of uncertainty—such as Script Concordance Testing (SCT)—have historically been dismissed as unfeasible due to immense administrative overhead. By integrating automated clinical assessment platforms, deans can completely bypass these resource barriers while simultaneously redirecting hundreds of faculty hours from manual administrative grading toward high-impact student coaching and programmatic implementation.
In a standard institutional setting, developing a single validated SCT requires recruiting a panel of 15 to 20 expert clinicians to manually construct a reliable scoring key, rendering the method non-scalable for large student cohorts. The Lecturio Healer application eliminates this barrier by providing immediate access to a pre-vetted library of over 130 highly specialized cases originally developed by the NEJM Group™, filterable instantly by organ systems, difficulty, and acuity.
Within the centralized Healer Educator Portal, institutional leaders gain access to granular analytical tracking metrics that redefine the residency training curriculum:
- Data Acquisition Efficiency vs. Thoroughness
- Lead and Differential Diagnostic Accuracy
- Illness Script Concordance
By establishing these uniform, AI-driven benchmarks, the platform provides a foundation for institutional faculty calibration. Instead of interpreting disparate, subjective clinical notes, educators are aligned around a shared mental model of a student’s reasoning trajectory. This centralized visibility ensures that automated metrics translate seamlessly into consistent, high-fidelity human coaching and targeted student remediation.
Rather than using open-ended conversational chatbots for patient history-taking, the platform utilizes specialized artificial intelligence models on the backend to deliver instant, real-time automated formative feedback on custom, free-text problem representations and management plans drafted by the student. This automated scoring aligns closely with advanced educational validation studies; A feasibility study published in Medical Teacher described a guideline-trained ChatGPT system used to generate SCT items and scoring keys in ophthalmology; physician reviewers provided generally positive feedback, though the evaluation involved only 10 respondents and the authors note AI cannot yet replace human expert panels
Proving the ROI: Standardized Outcomes and Reduced Faculty Fatigue
Implementing intelligent, data-driven clinical reasoning tools delivers a measurable return on investment by optimizing student training time and reducing institutional burnout metrics. Modern accreditation allowances encourage institutions to seek evidence-based interventions that balance training intensity with wellness. An RCT of AI-driven training in oncology residency demonstrated significant gains in clinical competence and longitudinal knowledge retention. Separately, the literature supports that reducing assessment burden on trainees may support wellbeing — though direct causal evidence linking automated platforms to student mental health preservation is not yet established.
As outlined in recent AI in medicine reviews, building an equivalent enterprise-level AI infrastructure entirely in-house introduces severe technical overhead, financial risk, and operational maintenance costs. By partnering with an established infrastructure like Lecturio, medical schools can access robust data mining platforms that support longitudinal competency tracking without overstretching faculty workflows.
Conclusion: Securing the Future of Clinical Competence
In an era defined by rapid medical knowledge expansion and severe global healthcare shortages, relying on passive lectures or delayed, subjective clinical evaluations places an institution’s academic reputation at risk. Adopting automated, step-by-step clinical reasoning quantification is a vital component of a modern assessment strategy to ensure uniform graduate safety and optimize overstretched faculty workflows.
Ready to see how Healer aligns with your school’s accreditation requirements? Schedule a tailored institutional demo with the Lecturio team today and secure your milestone outcomes.
Frequently Asked Questions
How does an automated clinical reasoning platform improve student board pass rates?
Turnkey applications strengthen a student’s underlying cognitive networks by continually contrasting their decision-making trajectories against expert clinician scripts. This active, repetitive retrieval practice ensures deep conceptual synthesis and guideline alignment, fostering superior long-term knowledge retention and reinforcing the cognitive foundations that underpin standardized test performance.
What metrics can deans use to track clinical assessment efficiency across clerkships?
The Healer Educator Portal tracks granular behavioral indicators, including data acquisition thoroughness, lead diagnostic accuracy, and illness script concordance keys. These metrics allow directors to identify specific competency gaps at an individual or cohort level long before high-stakes clinical rotations conclude.
Can a clinical reasoning tool alleviate faculty grading workloads significantly?
Yes, by utilizing specialized, pre-vetted AI scoring models, the platform provides real-time automated formative feedback on free-text problem representations. This removes the logistical burden of recruiting expert clinician panels to score script concordance items manually, saving hundreds of faculty hours.
