Introduction & The High Cost of “Digital Noise”
Medical schools are currently facing a quiet crisis of educational technology sprawl. As the number of unintegrated platforms grows, students face an invisible barrier to mastery: an overwhelming influx of digital logistics that fragments attention and drains mental energy. To understand why this matters so deeply for the future of healthcare, we must look at how the human brain processes information through the lens of Cognitive Load Theory (CLT).
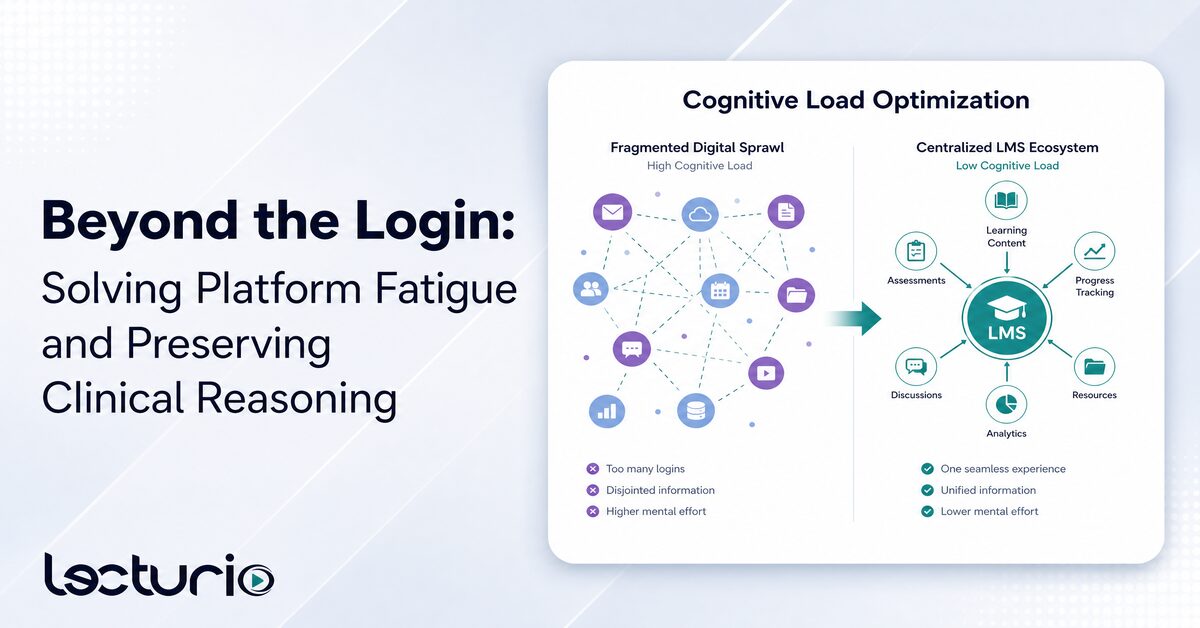
In educational psychology, cognitive load is divided into three distinct categories:
- Intrinsic Load: The inherent difficulty of the medical topic itself (e.g., understanding the coagulation cascade or fluid dynamics) which cannot be altered
- Germane Load: The productive mental effort a student expends to construct long-term mental schemas and build clinical reasoning skills
- Extraneous Load: The mental waste generated by the environment or instructions—such as broken links, multiple logins, and clunky interfaces—which adds zero educational value
The primary challenge of fragmented platforms is not that they inherently make medical concepts harder to learn, but rather that they artificially spike extraneous cognitive load. When a student is forced to navigate an unmanaged software sprawl, they fall victim to platform fatigue—a state of academic stress and cognitive exhaustion. This fatigue consumes finite working memory that could otherwise be dedicated to deeper learning processes, including the development of clinical reasoning and independent judgment.
The Central Thesis
Thoughtfully designed learning environments reduce unnecessary burden so learners can invest effort where it matters. Managing a modern medical curriculum requires a careful balance between technological innovation and cognitive capacity. Every year, higher education institutions navigate an overwhelming number of unique educational technology tools, turning purposeful instruction into distracting digital “noise”. For administrative leaders and deans balancing LCME Standard 6 compliance—which demands structured, coherent instructional design—this fragmentation introduces “digital logistics” that divert faculty time away from higher-value educational activities, such as direct mentorship, feedback, and hands-on clinical coaching.
This phenomenon is structurally verified by rigorous empirical data. A 2025 study of 160 healthcare students at one UAE college found that platform proliferation correlated with elevated digital cognitive load (r = 0.635); the authors note the single-site, all-female sample limits generalizability. This severe mental burden does not exist in a vacuum; studies show that multiple educational technology platform use negatively correlates with healthcare student well-being (r = -0.61), with digital cognitive load acting as the primary mediating mechanism.
Today, healthcare training programs routinely push students past a critical psychological tipping point by requiring them to navigate more than five distinct digital classes or platform frameworks simultaneously. High digital platform immersion contributes significantly to digital burnout and elevated stress among healthcare students. To preserve student resilience and protect the learning environment, institutional leaders must transition toward a centralized medical LMS ecosystem designed to optimize cognitive efficiency.
The Technical Fix: Frictionless Tool Interoperability
Centralizing the institutional learning management system (LMS) offers a scalable method to mitigate these digital demands and streamline course delivery. To eliminate the common, resource-draining problem of “lost password” support tickets and manual configuration errors, institutions are increasingly leveraging validated Learning Tools Interoperability (LTI 1.3 compliant) configurations, utilizing robust enterprise security frameworks like OAuth 2.0 and OpenID Connect.
Seamless LMS integration effectively embeds specialized digital ecosystems directly into the clinical workflow, drastically reducing the extraneous task-switching friction that prematurely exhausts a learner’s working memory.
However, as our central thesis reminds us, a streamlined technology architecture is an enabler, not the educator. Unintegrated digital tools present major institutional and operational risks. A comprehensive scoping review of LMS integration underscores that fragmented educational environments suffer from content validation failures due to severe time constraints, leaving faculty with an unsustainable administrative burden as they attempt to create and manually structure materials across disconnected systems. This ongoing fragmentation requires robust technical support and a unified single source of truth to ensure equitable, uninterrupted access.
As educational leaders optimize their systems, they must adopt a clear strategic approach: visibility comes before validation. You need to know what is actually being used to know what to validate for student growth. By housing resources within a centralized, institutionally validated medical LMS environment, medical schools can effectively automate reward schedules, track program performance metrics, and successfully clean up curriculum delivery —ensuring that tool interoperability serves to minimize extraneous logistical burdens so that the true work of pedagogy can take center stage.
The Efficiency Paradox: AI, “Deskilling,” and Scaffolding
The deployment of artificial intelligence in undergraduate medical training presents a profound efficiency paradox. In one comparative study of 79 Chinese medical students, those using generative AI tools completed biochemistry case assignments in under half the time (2.6h vs. 5.5h) and scored higher on exams. However, these rapid efficiency gains introduce severe pedagogical risks, such as deskilling—where previously acquired diagnostic skills erode due to reduced practice—and upskilling inhibition, which prevents students from forming new competencies because critical tasks are delegated entirely to automated software.
To manage this tension, we must refine how we view cognitive dual-process theory within digital environments. Experienced clinicians rely on a fluid interplay between fast, intuitive System 1 pattern recognition and slower, analytical System 2 systematic analysis. It is vital to note that System 1 reasoning is not inherently problematic; expert clinicians rely heavily on rapid pattern recognition to navigate complex clinical environments. The educational goal is not to eliminate intuition, but rather to help learners develop calibrated reasoning—the ability to fluidly move between intuitive and analytical processing, particularly recognizing when deliberate, slow System 2 reflection is required.
When unconstrained AI tools offer immediate, fully formed answers, they encourage novice students to favor quick System 1 shortcuts prematurely, causing them to entirely bypass the slower, cognitively demanding System 2 processes required to evaluate evidence and generate independent hypotheses. This unstructured integration can quickly create a “GPS effect,” where medical students blindly follow algorithmic prompts while completely losing their internal diagnostic map.
The risk here is not AI assistance itself, but the premature replacement of learner cognitive effort. Left unchecked, this dependency triggers “never-skilling,” meaning students fail to ever establish baseline mental architecture because automation substituted for their early cognitive efforts. It also fosters “mis-skilling,” leading to the uncritical acceptance of highly confident but clinically flawed or hallucinated algorithmic outputs.
To prevent this cognitive erosion, a modernized medical LMS must implement structural checkpoints and technical safeguards—known as digital scaffolding—grounded in Vygotsky’s Zone of Proximal Development. When intentionally designed, AI tools can actively support reasoning development rather than bypass it. Medical schools can look to emerging proposals like the M3RGE-AI framework (Responsible, Reliable, and Reflexive use of Generative AI) for direction here. Recently introduced as a conceptual model — not yet empirically tested — M3RGE-AI suggests structured, alternating AI-on and AI-off learning cycles to enforce Socratic interactions, positioning the software as a rigorous feedback loop rather than a passive shortcut. As its authors note, the framework is meant as a starting point for research and pilot programs, not a ready-made implementation guide.
Operationalizing the Curricular Shift
The structural differences between unmanaged digital sprawl and a centralized, integrated architecture demonstrate how infrastructure directly impacts the learning environment:
| Curricular Metric / Outcome | Fragmented Legacy State | Centralized Integrated State (LTI 1.3 Stack) |
| Task Efficiency & Workflow Speed | Variable, unmonitored, and prone to severe search and login fatigue. | Optimized; single sign-on (SSO) and direct workflow integration minimize navigation friction. |
| Digital Cognitive Load | High; driven by constant task-switching and credential friction. | Optimized; direct workflow integration minimizes extraneous fatigue. |
| Clinical Skill Protection | High risk of deskilling, never-skilling, and uncalibrated shortcut usage. | Managed via M3RGE-AI scaffolding and deliberate AI-off checkpoints. |
| Faculty Administrative Burden | High; spent troubleshooting access and manually structuring unverified data across systems. | Low; automated metrics and centralized institutional SSO tracking. |
| Accreditation and Quality Assurance | Fragmented local projects lacking standardized framework data. | Unified, evidence-based data streams supporting competency tracking. |
Data-Backed Decisions: From “Logins” to “Evidence”
To justify educational technology expenditures to institutional boards and university trustees, medical deans must pivot their evaluation frameworks away from superficial usage tracking. Traditional background data—such as basic logins, view counts, or clicks—merely proves a student opened a browser window, providing minimal insight into actual clinical competence. By transitioning from basic login tracking to genuine clinical evidence, institutions can deploy advanced Learning Analytics (LA) to measure deeper, multi-faceted markers of learner engagement.
Advanced Learning Analytics allow institutions to cross-reference basic background log statistics directly with predictive data points from interactive clinical case simulators, text analysis of summary statements, and time-on-task parameters to build precise learning trajectories. Utilizing an LTI 1.3 compliant platform architecture provides the enterprise-grade data pipeline needed to conduct continuous, rapid-cycle evaluation model tracking. Layering these integrated data streams directly with Student Information Systems allows deans to identify under-achieving or at-risk students long before end-of-semester exam failures occur.
The Educator-Led Element
While advanced analytics can identify behavioral patterns and generate early warning signals, data alone cannot replace human interpretation and context. Faculty judgment remains absolutely essential to understand a unique learner’s situation and provide meaningful, contextual coaching interventions. This approach takes the data back to what educators and students are actually doing, translating raw metrics into actionable, supportive mentorship.
Armed with this deep, context-specific institutional evidence, provosts can confidently prune their technical architectures, sunsetting non-compliant, redundant software applications to clean up the educational ecosystem.
Conclusion: A Foundational Enabler for Better Outcomes
Fostering authentic clinical engagement while protecting foundational reasoning from unstructured digital tools is no longer a minor curriculum adjustment—it is an absolute baseline requirement for the future of safe healthcare delivery. While building adaptive, scaffolded scenarios with appropriate boundaries requires deliberate administrative intentionality, the long-term institutional returns are undeniable. Deans and provosts who move decisively to address platform fatigue will reduce faculty cognitive fatigue, protect their students’ mental well-being, and ensure their graduates develop robust independent judgment.
Achieving a simplified, data-backed, and LTI 1.3 compliant medical learning stack is an important enabler for institutional efficiency. Yet, we must remember that professional formation and clinical development ultimately depend on a rich, interacting ecosystem of elements—including thoughtful curriculum design, dedicated mentorship, constructive feedback, and authentic clinical experiences. Technology clears away the operational friction; the human connection drives the professional transformation.
Ready to optimize your institutional edtech ecosystem, streamline faculty workflows, and safeguard your students’ clinical reasoning? Schedule a Demo with the Lecturio team today.
Frequently Asked Questions
How does a centralized LMS reduce digital cognitive load for medical students?
A centralized LMS minimizes digital cognitive load by combining multiple learning workflows, announcements, and assessments into a single user-friendly interface. This architecture eliminates task-switching friction, credential tracking fatigue, and interface navigation confusion, allowing medical students to focus working memory strictly on mastering complex clinical concepts rather than platform logistics.
What is the difference between deskilling and upskilling inhibition in medical education?
Deskilling refers to the gradual erosion of existing diagnostic acumen and technical competencies when a student over-relies on automated systems instead of actively practicing clinical reasoning. Upskilling inhibition represents a developmental barrier where a student misses the opportunity to form entirely new advanced cognitive frameworks because an AI tool supplies fully formed clinical solutions too early in the learning process.
How can institutions use learning analytics to identify at-risk medical students?
Institutions can identify at-risk students by continuously monitoring integrated parameters within the LMS, such as forum discussion participation, time spent on case simulations, and formative quiz scores. By tracking these continuous behavioral streams, educators can detect declining engagement patterns and provide targeted pedagogical support long before traditional summative exams take place.
What safeguards protect clinical judgment from automation bias?
Enforcing structured pedagogical frameworks like M3RGE-AI protects clinical judgment by implementing alternating AI-on and AI-off learning cycles. Incorporating unassisted diagnostic tasks, Script Concordance Tests, and “AI-wrong” OSCE stations ensures that senior students build independent hypothesis-generation habits and learn exactly when to override flawed algorithmic recommendations.
