Playlist
Show Playlist
Hide Playlist
Vertigo: Types

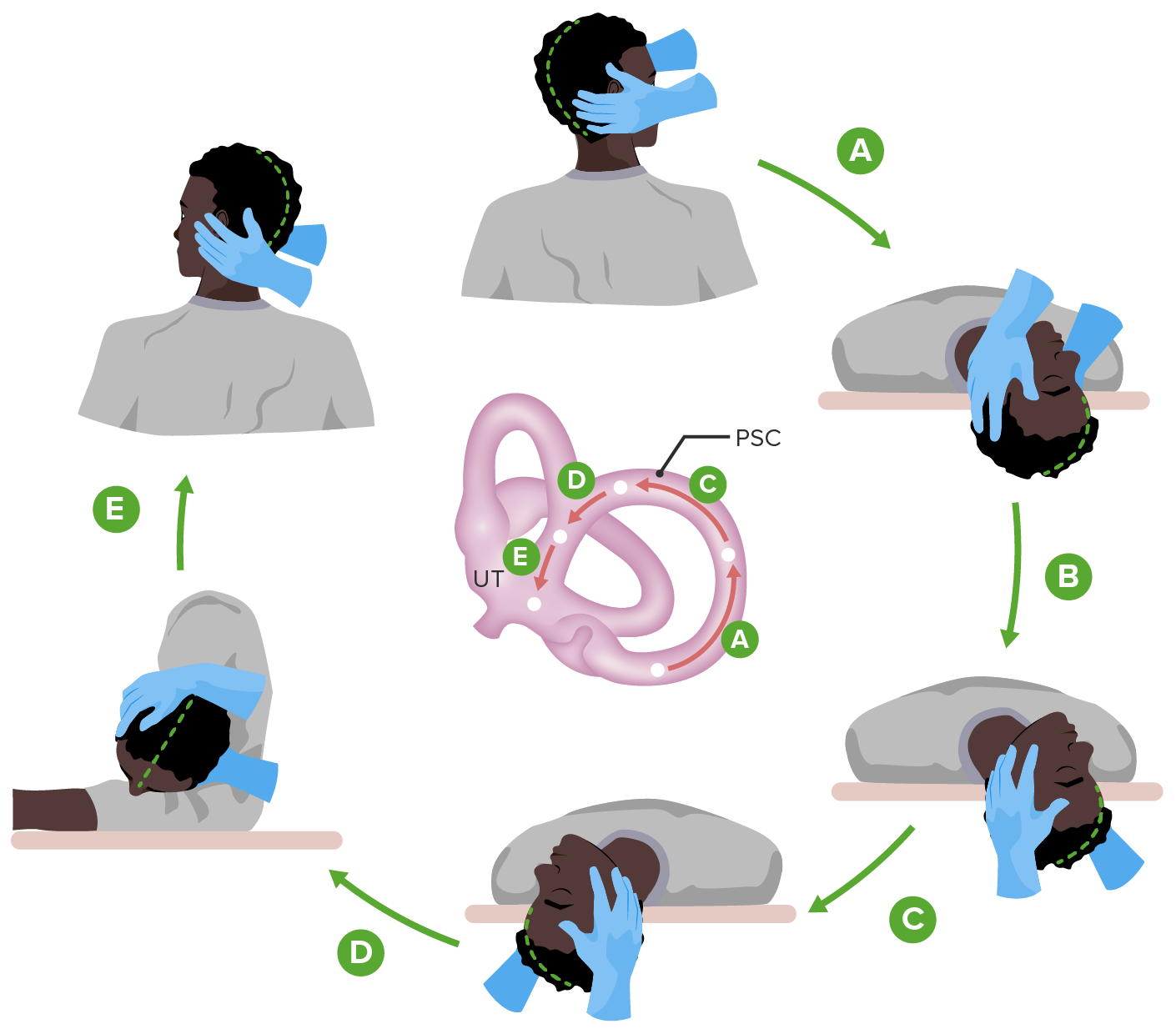
00:01 This algorithm or flow diagram really helps me to understand the types of diagnoses that we need to be concerned about for any patient presenting with vertigo. 00:10 The first thing we look at is the timeline of onset. 00:13 Some patients present acutely over hours with new onset vertigo. 00:18 Rooms spinning and them spinning about the room. 00:20 And it remains persistent over time. 00:23 We call that acute persistent vertigo, or the acute vestibular syndrome. 00:28 And we'll talk in a subsequent lecture about how to approach those patients. 00:33 Other patients present acutely with sudden onset of vertigo. 00:36 But it's episodic over time, as we saw in this case, with periods where there's intense vertigo, followed by remission where the patient is normal. 00:47 And then finally, we can see causes of chronic onset vertigo. 00:50 They're present slowly over time often with associated cerebellar findings. 00:54 Nausea or vomiting, or problems with balance, or coordination, or postural tone. 00:59 And there's a certain set of conditions that we would consider for chronic onset vertigo. 01:04 So the timeline is onset is critical in evaluating these patients and honing in on a precise differential diagnosis. 01:11 When we think about episodic vertigo, those paroxysmal paroxysms, those episodes of vertigo can be positionally provoked, or spontaneous. 01:19 And that can also help us in the differential diagnosis. 01:23 So let's think more about each of these buckets, each of these categories of vertigo. 01:28 For chronic onset vertigo, we think about medications. 01:31 They're one of the most common causes of chronic vertigo suffered by patients, and many medications can cause room spinning or spinning about the room. 01:39 And an adjustment and dose or removal of those offending medications is the treatment of choice. 01:44 We also think about mass lesions. 01:46 Slowly growing mass lesions in the posterior fossa, either a tumor, an infectious process, or an abscess, can present in this way and are important to to evaluate. 01:56 We think about mass lesions within the cerebellum, and brainstem and around the vestibular nuclei, and vestibular system, as well as those on the vestibular nerve like vestibular schwannomas, which can present with hearing loss and varying degrees of vertigo. 02:12 When we think about acute episodic vertigo, that's vertigo that caused that comes in episodes and may be positionally provoked, or spontaneous. 02:23 That categorization is important. 02:25 There are certain conditions that are provoked by selected maneuvers. 02:29 Head movement is one of the most common propagating factors and we see that with BPPV. 02:34 But we can also see positionally induced vertigo, that's vertigo that worsens with standing with orthostatic hypotension, and vertebrobasilar insufficiency. 02:43 Were raising of an arm or activation of an arm can set off an episode of vertigo. 02:49 That's different from spontaneous onset episodic vertigo, which would be seen in the case of vestibular migraine episodes of intense vertigo that just come on spontaneously. 02:59 We can see this with TIAs, arrhythmias, ACS or Acute Coronary Syndrome, and with manures disease where we see prominent hearing loss, and sometimes tinnitus. 03:11 Let's talk about a couple of examples of acute episodic vertigo that you should know clinically when evaluating patients or vignettes. 03:19 The first as we saw in this case is BPPV. 03:22 This is acute onset vertigo that comes and goes over time with episodes of relapses and remissions. 03:29 There recurrent episodes of severe vertigo often the vertigo is very severe for patients and may be associated with nausea, vomiting, and problems with balance and walking during the episode. 03:39 This is typically provoked by head turning. 03:42 On examination, we see an associated torsional nystagmus. 03:45 That's a rotary nystagmus of the eyes, as well as an upbeat nystagmus. 03:50 And that combination of torsion and upbeat nystagmus with head turn is diagnostic of this condition. 03:56 Episodes of vertigo can be induced by maneuvers and specifically the Dix-Hallpike maneuver, where the patient is brought from a seated position to align position, and then turning the head, and lowering it below the bed can induce that onset of torsional and upbeat nystagmus, and intense vertigo for the patient. 04:14 And pathologically, what we see going on in the vestibular apparatus to cause this is displacement of calcium oxalate crystals within the semicircular canals. 04:25 Those are dislodged. 04:26 They circulate in the semicircular canals and can cause a sense of movement without movement actually occurring. 04:33 That process can drive these episodes of vertigo. 04:36 Patients can have clusters of episodes when those calcium oxalate crystals get dislodged, that can remit for sometimes months or years and then recur over time. 04:47 And to treat this condition we can use medications. 04:50 But the best treatment is a physical exam maneuver the Epley or Brandt-Daroff maneuver, which maneuver those calcium oxalate crystals to benign location in the semicircular canal. 05:03 That treatment can be curative at the time of the intervention. 05:06 And so that's something we do in the clinic or in the emergency department to treat these patients that's after a diagnosis has been made, or would consider vestibular rehab for long-term management with repeated maneuvers over time. 05:20 So if BPPV is the example of acute episodic vertigo that is provoked by head movement. 05:26 Vestibular migraine is acute episodic vertigo that occurs spontaneously. 05:31 This is a headache syndrome. and some patients have headache. 05:35 Others have an acephalgic presentation primarily with vertigo, and very minimal or no head pain. 05:42 Patients describe associated dizziness, vertigo that may proceed or occur during the headache phenomenon. 05:48 This occurs in episodes like any migraine. 05:51 Patients have periods of two to 72 hours of vertigo, headache, and disability. 05:58 And this is followed by periods of remission or headache free, and vertigo free intervals. 06:03 It may or may not be associated with actual head pain. 06:06 And this is important. 06:07 Patients who present with vertigo and head pain we think about migraine, but we need to consider those acephalgic presentations. 06:15 Ultimately, this is a condition that responds to antimigraine treatments. 06:21 And then our last bucket of conditions are the acute persistent vertigo's. 06:27 This is acute onset vertigo room spinning that doesn't come and go in waves and episodes but is persistent when it starts. 06:35 That acute vestibular syndrome is a characteristic syndrome that requires a different evaluation from our other patients with vertigo that we'll discuss in a future lecture. 06:44 Our key goal as clinicians is to differentiate peripheral vertigo from central vertigo. 06:50 And that is a key process for evaluating patients with the acute vestibular syndrome. 06:55 That's not our goal for evaluating other causes of episodic vertigo. 06:59 And this underscores the importance of characterizing both the timeline of onset whether it's acute or chronic, and the evolution over time, whether the patient suffering persistent vertigo, as in the acute vestibular syndrome, or episodes of paroxysms, as in the case of BPPV, and vestibular migraine.
About the Lecture
The lecture Vertigo: Types by Roy Strowd, MD is from the course Vertigo, Dizziness, and Disorders of Balance.
Included Quiz Questions
Which statement is the most accurate with respect to vertigo classification?
- Vertebrobasilar insufficiency can be induced by arm raising.
- Acute episodic vertigo is usually known as acute vestibular syndrome.
- Vertebrobasilar insufficiency is classified as acute episodic vertigo.
- Ménière’s disease is classified as acute vertigo with positional episodes.
- Vestibular migraines can be induced by head turning.
Which statement is the most accurate with respect to benign paroxysmal positional vertigo?
- Head turning can provoke an episode.
- There are no pharmacological treatment options.
- Benign paroxysmal positional vertigo usually results in hearing loss.
- Benign paroxysmal positional vertigo is treated with the Dix-Hallpike maneuver.
- Benign paroxysmal positional vertigo presents with a characteristic downbeating nystagmus.
Which of the following is the most accurate with respect to vestibular migraines?
- They can have an associated headache.
- Treatment includes the Epley maneuver.
- They are refractory to typical migraine medications.
- They are classified as continuous vertigo with an acute onset.
- They can be provoked by certain head movements.
Which statement is the most accurate with respect to acute vestibular syndrome?
- Acute vestibular syndrome can be precipitated by a brainstem stroke.
- Episodes can be caused by raising of the arms.
- Acute vestibular syndrome is always caused by peripheral vestibular system pathology.
- Acute vestibular syndrome can be induced by a specific head maneuver.
- Acute vestibular syndrome is categorized as episodic vertigo with an acute onset.
Author of lecture Vertigo: Types

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
