Playlist
Show Playlist
Hide Playlist
Usual Interstitial Pneumonia (UIP): Signs and Symptoms


-
Slides RestrictiveLungDisease RespiratoryPathology.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
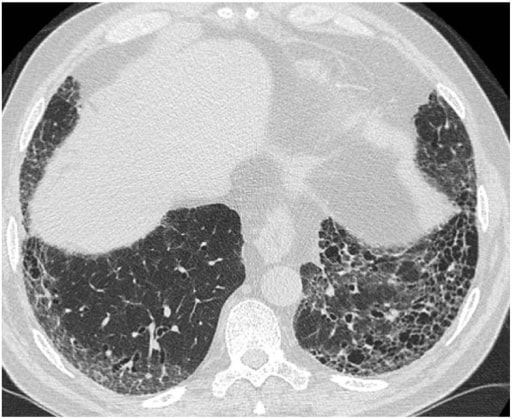
00:01 Insidious onset, progressive dyspnoea because of that increased fibrosis. Imagine that this fibrosis that’s continuing and then what happens? A dyspnoea at first only with exertion. 00:12 As the fibrosis gets worst then what would then happen to that dyspnoea? Could occur even at rest and what happens to exercise tolerance? All downhill. Dry, non-productive cough, why? The reason I’m shaking my head is this is non-productive, not in the alveoli. 00:33 Everything that we talked about here prior, when we’re looking at COPD, what kind of cough was that? Chronic bronchitis, bronchiectasis, asthma, there you go that was productive cough. Quite a bit of mucous. That was in the airways and the alveoli and such. This is in the? Good, interstitium. And so therefore, the cough would be present because irritation but not necessarily productive. 01:00 Physical examination. Dry “Velcro” crackles on pulmonary auscultation because of interstitial involvement. Chronically over a period of time digital clubbing, obviously cyanosis. What about your pulmonary function test? Predict what you’re going to see first, close your eyes, let me walk you through this. What about total lung capacity? Decreased. 01:23 What about force vital capacity? Decreased. What about FRC? Decreased. What about DLCO? Decreased. What about your FEV1/FVC ratio? Not decreased. Obviously, restrictive pattern. 01:39 Radiology, so therefore, upon your X-ray and imaging, what are you going to find on chest X-ray? If it’s the interstitium that’s being affected it is not the alveoli that you’re paying attention to, it is the parenchyma. On chest X-ray this type of pattern that you find with the meshwork of your parenchyma is known as reticular. The very beginning of pulmonology we specifically went through imaging studies, and I showed you the different patterns, this would be a good time for you to go back and take a look at that review please. For example in chest X-ray it is called reticular. On CT it is called? Good, ground glass. So, fibrosis honeycombing appearance, most notably at the lung bases, sub-pleural type of distribution. On CT this would then be referred to as being your ground glass. 02:32 Perfect CT of what we’re seeing here with ground glass type of appearance. The CT image shows basal predominant, peripheral predominant reticular abnormality and traction, bronchiectasis and a lot more of your honeycomb. Take a look at the base, you see the septae, you can clearly see that this would be a honeycomb type of appearance and reticular technically and also called as being ground glass in the parenchyma. 03:04 Now, with usual interstitial pneumonitis diagnosis. Biopsy not always required if the epidemiology fits. So, if your patient is a little bit older and you find that the exercise tolerance is decreasing, you could not find any underlying issue, then please understand that you should be thinking about usual interstitial pneumonitis, pathology. Clinical diagnosis would be your idiopathic pulmonary fibrosis. Trust me, you’re not going to find two answer choices where A is going to be usual interstitial pneumonitis and B is idiopathic pulmonary fibrosis. Clinically, that doesn’t achieve anything, it’s just ridiculous. So, if you get any questions, just think, the person that query that question has no idea what they’re doing. So anyhow, pathology shows patchy interstitial fibrosis with area of fibroblast foci, that should make perfect sense. If you’re depositing, well, if you’re creating fibrosis does not mean that position of collagen. Who’s coming in? Fibroblast. 04:06 So, from your histology lectures, you should definitely know what a fibroblast looks like, okay, especially for such instances. Also, what ends up happening is you find these cystic areas around it. Well, this is a highly magnified type of specimen, but what is circled here would be the cystic spaces. If you were to blow out, okay, on your chest X-ray or maybe perhaps even CT, then you’d find the surrounding area where there would be increased fibrosis and thickened septae, okay, honeycombing. 04:39 Okay. Now, prevention, quite difficult, no proven therapy as well. Oxygen supplementation to treat hypoxemia. Please understand that you’re giving oxygen even though there might be a decrease in DLCO. Only small percentages respond to steroid therapy. Lung transplantation might be actually your next step of management here. Okay, so, that’s crazy. Steroid therapy, most likely would not, many of those likely have connective tissue diseases, right? So, therefore, by giving steroid, it wouldn’t treat the rheumatoid arthritis per se, right? Next step of management, transplantation.
About the Lecture
The lecture Usual Interstitial Pneumonia (UIP): Signs and Symptoms by Carlo Raj, MD is from the course Restrictive Lung Disease.
Included Quiz Questions
Which of the following is unlikely in usual interstitial pneumonitis?
- Cough with sputum
- Clubbing
- Cough without sputum
- Cyanosis
- "Velcro crackles"
Which of the following pulmonary function tests is not found in usual interstitial pneumonitis?
- Decreased FEV1/FVC ratio
- Decreased DLCO
- Increased FEV1/FVC ratio
- Decreased TLC
- Decreased FRC
Which of the following CT scan findings is not seen in idiopathic pulmonary fibrosis?
- Basal predominant calcification abnormality
- Traction bronchiectasis
- Basal area honeycombing
- Peripheral predominant reticular abnormality
- Basal predominant reticular abnormality
Which of the following is a classic feature seen in the pathology of usual interstitial pneumonitis?
- Patchy interstitial fibrosis with areas of fibroblast foci and cystic areas of honeycombing
- Patchy interstitial calcification with areas of fibroblast foci and cystic areas of honeycombing
- Patchy interstitial fibrosis with areas of fibroblast foci and cystic areas of vascularization
- Patchy interstitial fibrosis with areas of calcified foci and cystic areas of honeycombing
- Patchy interstitial fibrosis with areas of fibroblast foci without honeycombing
Which of the following is correct about usual interstitial pneumonitis?
- Reticular pattern on CXR and honeycombing on CT
- Reticular pattern on CXR and calcification on CT
- Calcification on CXR and honeycombing on MRI
- Granulomatous pattern on CXR and honeycombing on CT
- Reticular pattern on CXR and honeycombing on MRI
A 45-year-old man with a history of usual interstitial pneumonitis is started on oxygen therapy to manage his dyspnea. He returns to the clinic with persistent symptoms. Steroids are prescribed. If there is no improvement in his symptoms, what would be the most appropriate next step in the management of his condition?
- Lung transplantation
- Antibiotics
- Noninvasive ventilation
- Increase the dose of oxygen.
- Increase the dose of steroids.
Author of lecture Usual Interstitial Pneumonia (UIP): Signs and Symptoms

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
