Playlist
Show Playlist
Hide Playlist
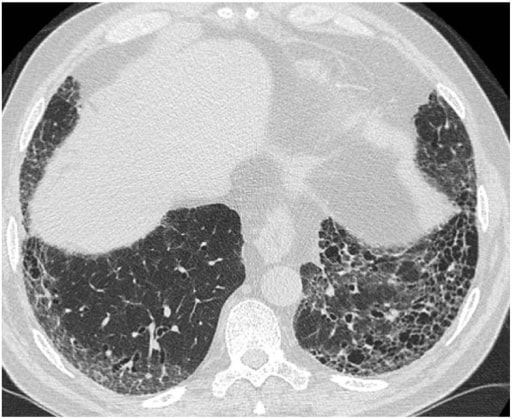
Usual Interstitial Pneumonia (UIP): Pathogenesis


-
Slides RestrictiveLungDisease RespiratoryPathology.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
00:01 Now, usual interstitial pneumonia, what are we looking at? It’s idiopathic remember that’s the clinical diagnosis that you’ve taken out of this. Leading to what? Fibrosis of the lung parenchyma. What happens? Your DLCO is then going to decrease and what happens to your A-a gradient? Rule of thumb, definition that we walked through already, increased. Good, pulmonary. The fibrosis increase the distance over which the oxygen has to be properly transported from one side of the membrane to the other and that is then impaired. 00:33 What’s the test that you’re doing here please? Good, your DLCO. We talked about hypoxia and if this occurs over a long period of time what are you going to find with your nails, fingers? Digital clubbing, right? Cyanosis, yeah of course but that you know, that occurs even acutely. Chronically, you see clubbing, which is bulbous enlargement of the ends of the fingers or toes. The fibrosis also decreases the compliance., what does that mean? It’s becoming stiffer, so therefore restriction of entry. And usual interstitial pneumonitis is a disease of older patients as you can expect because of increased fibrotic deposition. 01:16 Now, consider diffuse lung disease differentials. Make sure it’s not associated with connective tissue disease and that’s important so whenever there is the issue with fibrosis in the parenchyma rule out any drugs or maybe occupational exposure, and we’ll talk about more of this later on when we start addressing what’s known as hypersensitivity pneumonitis, is that clear? So, usual interstitial pneumonitis, sure you’ll have your fibrosis but with this fibrosis well, as you’ve said the clinical pattern here is going to be your idiopathic pulmonary fibrosis and then your pathologic pattern would be usual interstitial type of pneumonitis. 01:57 Go back to that table and take a look at the two categories. Clinical pattern, pathologic pattern. Clinical pattern, pathologic pattern. Do not be confused between the two. 02:06 Now, consider the diffuse lung disease differentials, what are these? Well, you may require lung biopsy. Keep in mind that the pathology of usual interstitial pneumonitis which is the fibrosis is the final common pathway of severe lung disease, isn’t it? so often times when you find this fibrosis apart from just automatically giving it a label of idiopathic, was there an underlying issue, was there recurrent bout of whatever lung disease resulting in fibrosis? UIP, IPF will go hand in hand. Now, 80% or greater would be of sporadic. Familial, smaller percentage. The mucin gene that you want to know, MUC at least be able to identify that and there’s also telomerase plus surfactant mutations as well seen mostly in older patients.
About the Lecture
The lecture Usual Interstitial Pneumonia (UIP): Pathogenesis by Carlo Raj, MD is from the course Restrictive Lung Disease.
Included Quiz Questions
Which of the following is a gene associated with idiopathic pulmonary fibrosis?
- MUC5B
- MUC5A
- SS-A
- SS-B
- CFTR
Which of the following is FALSE about usual interstitial pneumonia?
- It is a connective tissue disease.
- It is idiopathic.
- It involves inflammation with subsequent fibrosis.
- It is associated with impaired oxygen diffusion,
In the context of usual interstitial pneumonitis, which of the following is a late clinical feature associated with chronic hypoxia?
- Digital clubbing
- Immediate cyanosis
- Sudden increase in Forced Expiratory Volume in 1 second (FEV1)
- Decreased fibrotic deposition
- Increased lung compliance
A 65-year-old man is brought to the ER with difficulty breathing. His pulmonary function tests show a decrease in total lung capacity (TLC) and an increase in the ratio of the forced expiratory volume in the first second (FEV1) to the forced vital capacity (FVC) [FEV1/FVC]. On examination, digital clubbing is noted. Which of the following tests is essential to demonstrate an impaired diffusion capacity of oxygen in this condition?
- DLCO
- PET scan
- CT scan
- Bronchoscopy
- Lung biopsy
Author of lecture Usual Interstitial Pneumonia (UIP): Pathogenesis

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
