Playlist
Show Playlist
Hide Playlist
Typical and Atypical Ribs

-
01 Slides Cymet Rib Cage Region General Principles.pdf
-
Reference List Osteopathic Manipulative Medicine.pdf
-
Download Lecture Overview
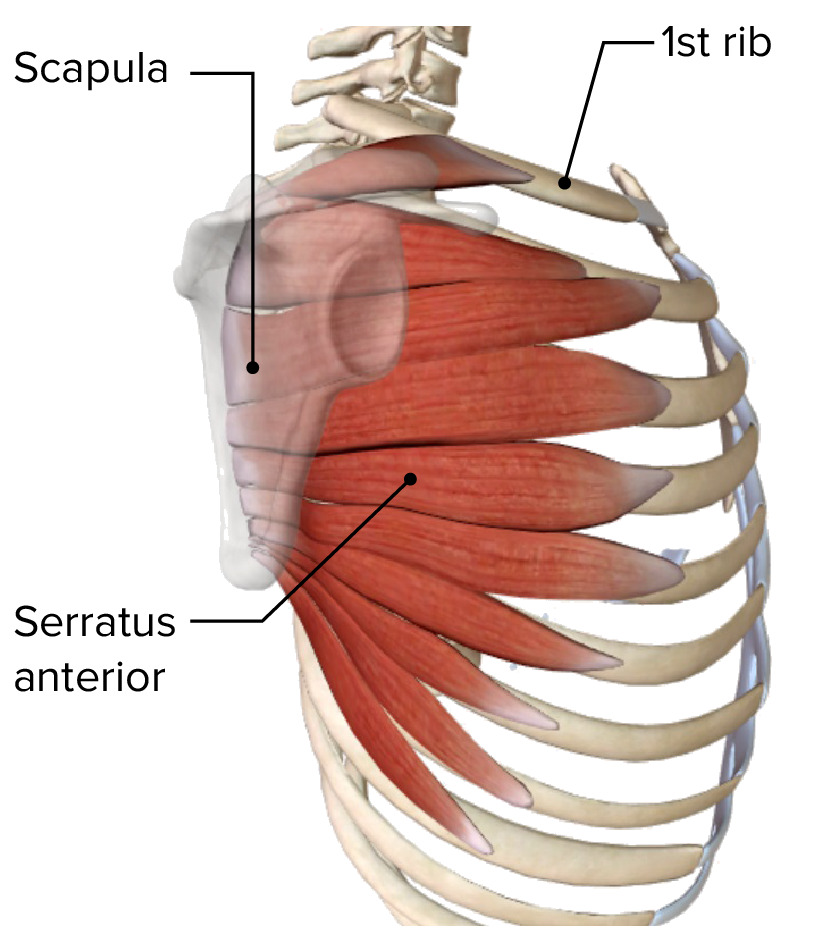
00:00 Ribs 3 through 9 are typical ribs. They have a similar structure where the rib starts in the back by the spine and the head of the rib is going to articulate with the vertebrae and then you’re going to have the tubercle attached to the vertebrae above where the head is and then come around, curved. Again start at, let’s say, rib 6, T6 attached to T5 as well. It will then come down and then come up but not as far as it would be from where it starts. That's the general structure of the typical rib and the neck and the tubercle articulate with the transverse process and costovertebral ligaments and the ligaments cement the head of the rib in place and the tubercle is tightly held next to the vertebrae. Again, this is why in a trauma you are at risk for fracturing or injuring the ligaments and these are not easy to image and not easy to see on x-rays or CAT scans or MRIs. So, the flat curved nature of the ribs is effective for motion but it does have some downsides and that it's susceptible to trauma, susceptible to rapid changes and speed or motion. 01:30 Here is another example of typical rib just so you can see what they look like and again they get larger as you get down to T10. T10, T11 and T12 are atypical ribs. So the atypical ribs. 01:44 What does it mean? They’re part of the rib cage, they’re part of the structure that encases the chest wall cavity. The first rib is the shortest rib. It’s got the greatest curvature, it’s also flat without an angle or costal groove and it has a single facet so it articulates only with T1. It doesn't go up to C7. It doesn't attach to anything but T1. The second rib, the costal cartilage, has 2 demifacets that attaches to the manubrium and that's going to also move a little bit differently and when we talk about motion, we'll talk about the pump handle motion of the upper ribs. Part of that has to do with the structure of the ribs at top that dictate the motion. 10 through 12 also will only have one facet and attach only to the one level of vertebrae. So it isn’t stabilized, it isn’t braced and the motion has more ____ is more likely to change. T11 and T12 have no necks, no tubercles, no attachment to the rib above. Again another picture of an atypical rib showing where the subclavian vessel will be and the muscle attachments that will move and stabilize the bone. The atypical ribs will include the upper and the lower ribs, ribs 1 and 2; ribs 10, 11 and 12. Rib 1 is where the thoracic inlet is and you have to be very conscious of that because you'll see a lot of complaints, a lot of issues with neuromuscular dysfunctions. The manubrial attachment is usually rib 2. Again, rib 2 still comes down a little bit and comes back up and attaches by the manubrium. Rib 10 is typical in structure with the atypical articular facet again attaching to 1 vertebra and not always attaching to the vertebrae above it. 11 and 12 are floating ribs with no anterior attachment. It’s going to have caliper motion, it’s not going to have the pump handle of the upper ribs or the bucket handle of the lower ribs that we’ll talk about a little later. So each rib again has a slope and this is meant to slow down. Think about the rib cage and understand that when you’re looking at the body there's somewhat of a forward bending slope to it, somewhat of an asymmetry in the body. We get used to looking at people like this because people hold their ribs the same way they hold their chest the same way and in looking at it again higher in the back, lower and then coming up. There is some smoothness to it but if you trace a single rib it will be helpful. So take a second, trace your rib from the back to the front and get a good sense of the curvature. Then turn the patient around and trace the rib again from the back coming down and then coming back up and do this with palpation, feel the rib, feel where it's coming to and get a sense of how the change occurs. Why is this important when we get to inhalation lesions? Someone breathes in and they can't fully exhale. it's restricted that’s going to matter and understanding the normal is going to help. Getting the attachments will help with the motion. The manubrium is at the level of T3/T4 because again it's coming down and not coming back as far up. You are going to have the jugular notch there, you’re going to have the you’re going to have the clavicular notch where the clavicle attaches and you’re going to have the costal cartilage of the 1st rib and the clavicle attaching to the manubrium. When you get to the sternum, you want to notice the angle of Louis. By 30 years of age, that’s set. You are going to have some hypertrophy, bony enlargement after that but you’re not going to have the same trabecular matrix of the bone, you’re not going to have the same sponginess to the bone. It is more likely to fracture, more likely to separate and more likely for people to have medical issues after 30 years of age and the sternal angle, the angle of Louis, will give you a sense of is it formed, is it solidified, has the organs stopped developing and what age is it? When we talk about aging, yes the sacrum, the size and shape is one of the most sensitive but the manubrium also has a different size and shape in men and women. The sternum larger, thinner and narrower than the manubrium so it starts to taper down from level 5 to 9 and then when you get to the xiphoid it gets even smaller. Originally, the sternum is in 4 separate pieces but again it ossifies by 30 years of age and we call the sternal pieces sternebrae. I want to talk a little bit more about the sternomanubrial junction because again we look at it all the time, we notice it, it's very evident and it does give us some information. It does tell us what’s going on with that joint, how good is the motion, how fluid is the motion, how stuck is the motion, how likely is this person to develop breathing problems because their rib cage is not healthy, not easily moving, not smoothly moving. So, you look at the sternomanubrial junction and we often test and check the sternoxiphoid junction to see if the articulation has solidified and is moving or not. While the xiphosternal junction is cartilaginous, it is a synchondrosis of bone-on-bone joint that moves somewhat but not very much and the sponginess, the motion, is a general sign of how easily it is to move and how healthy the joint is. In older people again, once it's ossified the motion is going to be less and you may feel some crepitus, you may feel decreased motion and even some tenderness to the musculature when you try and move. Let’s examine the xiphoid process now because it's the bottom of the sternum, it's the smallest part of the sternum and it's also variable, it's thinly elongated, it sometimes bends inward, it sometimes has extra pieces, sometimes you get ossicles formed but you can tell if it's tender or if it's easily moving or not easily moving. It tends to ossify by 30, sometimes 40 years of age and tends to stop changing as rapidly after that and doesn't have as much of an organ function. So it's just something to be aware of. It will give you a clue as to whether or not there’ll be breathing problems, breathing sticking or breathing ease. It's also a marker for checking the liver, checking the stomach and seeing where organs are and for reproducibility of the exam and when you think of the thorax again we tend to look at the rib cage but the strut of having the clavicle and the sternum also affects motion and mobility, it affects comfort levels and it also connects to the sternum which is part of how it affects motion and breathing.
About the Lecture
The lecture Typical and Atypical Ribs by Tyler Cymet, DO, FACOFP is from the course Osteopathic Diagnosis of the Ribs. It contains the following chapters:
- Typical Ribs
- Atypical Ribs
Included Quiz Questions
Which of the following parts of the typical rib is thin, flat, curved and has a costal groove on the inferior edge?
- Body/shaft
- Head
- Neck
- Tubercle
- Facet
Which of the following parts of the typical rib is round and knob-like and articulates with the vertebrae?
- Head
- Neck
- Tubercle
- Body
- Shaft
Which of the following atypical ribs has the greatest curvature, is flat and has a single facet?
- Rib 1
- Rib 2
- Rib 11
- Rib 10
- Rib 12
Which of the following atypical ribs has an atypical articular facet structure?
- Rib 10
- Rib 2
- Rib 1
- Rib 11
- Rib 12
The sternal angle of Louis is found at the level of the 2nd pair of costal cartilages; At which intervertebral level is the sternal angle of Louis found?
- 4th disc space
- 3rd disc space
- 5th disc space
- 2nd disc space
- 6th disc space
Author of lecture Typical and Atypical Ribs

Tyler Cymet, DO, FACOFP
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
very clear liked it very much thank you so much
