Playlist
Show Playlist
Hide Playlist
Toxic and Metabolic Causes of Myelopathy

-
Slides Diseases of the Spinal Cord.pdf
-
Download Lecture Overview
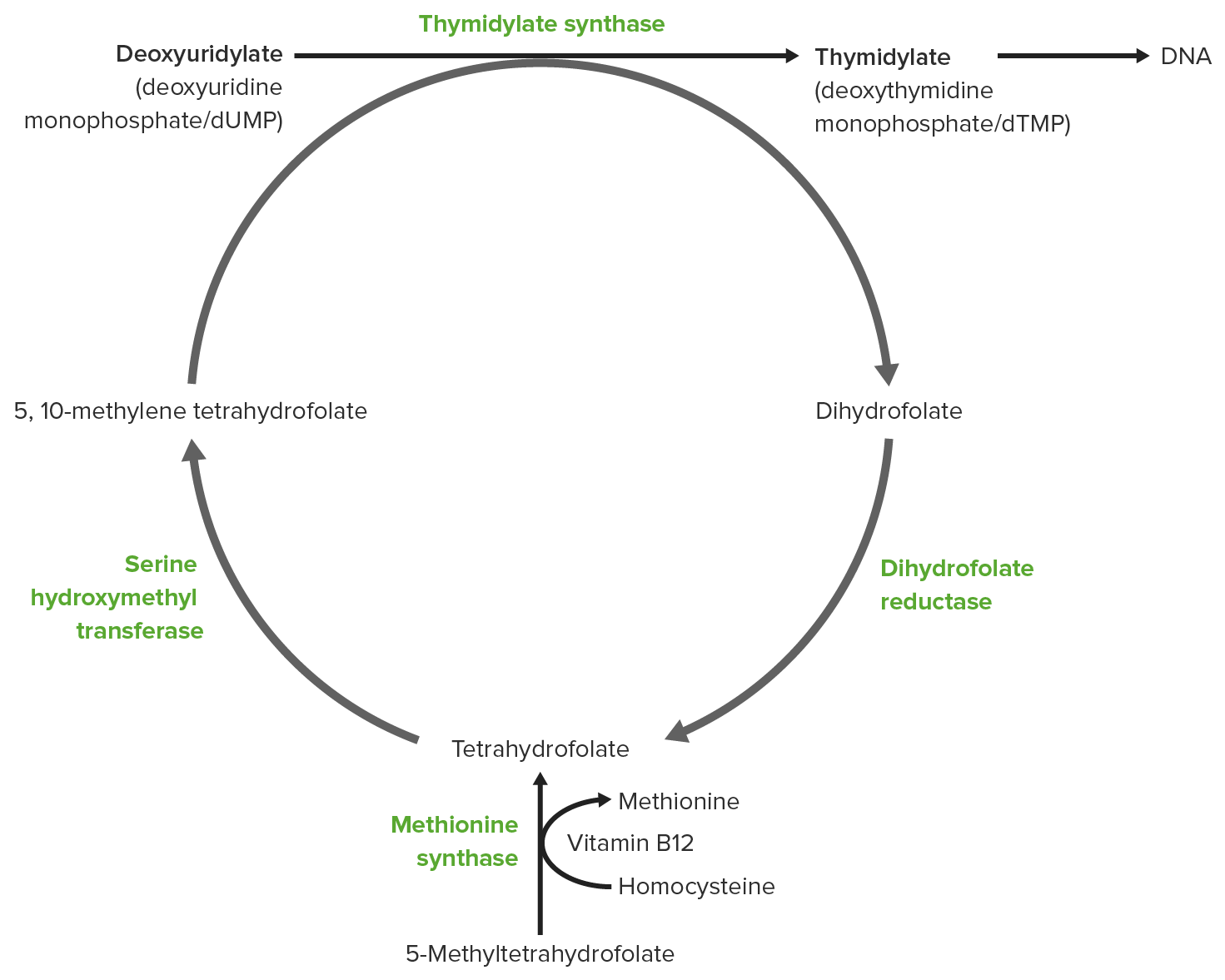
00:00 So let's talk a little bit more about this 4th category of myelopathies. Toxic metabolic is a common cause of a normal MRI in a patient presenting with myelopathy. 00:13 There are other causes, but let's focus on some of the toxic and metabolic etiologies. 00:18 Typically, these patients will present, as in our case, with symptoms that localize to a spinal cord pathology but the MRI may be normal or show some characteristic toxic metabolic changes. And we want to think about things like metabolic disorders, toxic ingestions, as well as infections, vascular etiologies, and potentially a functional etiology as well. When we think about some of the toxic metabolic myelopathies, there is a number. Let's walk through a typical list of things that we want to include in the differential diagnosis for these patients. vitamin B12 deficiency, as was present in our case, is a common condition affecting the spinal cord. Neurologic features, signs, and symptoms include a myelopathy at presentation. Sometimes we can see myeloneuropathy or both a spinal cord and peripheral nerve pattern. Patients may have memory loss, psychosis, or orthostatic hypotension owing to other involvement of nerves in the central nervous system as well as autonomic nervous system. Some of the common causes for vitamin B12 deficiency include malabsorption, atrophic gastritis, an autoimmune phenomenon or condition pernicious anemia as well as other gastrointestinal disorders. To make this diagnosis as with many of our metabolic deficiencies, we're going to test the serum for vitamin B12 when we see low vitamin B12. In addition, methylmalonic acid and homocysteine, which are intermediate metabolites in B12 processing, are elevated. And treatment is to replace the metabolite that is deficient and in this case that's B12. Folic acid is also an important cause of a toxic metabolic myelopathy. Folate deficiency can present very similarly to vitamin B12 with all of those same typical features. Causes include alcoholism, chronic GI disorders, and other problems with folate absorption. 02:17 Again, testing here is serum folate levels and we look at serum folate in the red blood cells and treatment is supplementation with folic acid. Importantly, copper in copper deficiency is another cause of toxic metabolic myelopathy. Again, these patients present very similar to vitamin B12 deficiency with a myelopathy or myeloneuropathy. 02:40 So again, problems with the spinal cord or spinal cord and peripheral nerve. Common causes include excessive zinc ingestion. Zinc can chelate copper, bind up copper and result in a copper deficiency and precipitate this disorder. Denture cream has historically used zinc and so we can see copper deficiency in those patients as well as gastric surgery or other GI conditions. As with the other conditions, we look at testing in the serum. Serum copper, ceruloplasmin, as well as 24-hour urine copper can be helpful in these patients. And when zinc toxicity is suspected, serum zinc levels. 03:20 Treatment includes supplementation with copper to replete the copper that is deficient. And then lastly, vitamin E deficiency can present with a myelopathy. This can actually be a combination of an ataxic myelopathy. So we see myelopathy, neuropathy, similar to the other conditions but we can also see ataxia as well as pigmentary retinopathy and visual changes. Potential causes of vitamin E deficiency include chronic cholestasis, pancreatic insufficiency. This is a fat soluble vitamin and so we can see conditions that affect that causing this presentation. Testing includes serum vitamin E looking for deficiency of vitamin E and treatment is supplementation. 04:05 There are also a number of toxins that can present with a myeloneuropathy presenting very similar to B12 deficiency; nitrous oxide, heroin, radiation and a number of other things. Nitrous oxide is particularly interesting in that it can precipitate a rapid B12 deficiency. So this looks all the world like B12 deficiency with that subacute combined degeneration of the corticospinal tract and dorsal columns, but we see borderline low levels of vitamin B12. What helps to establish this diagnosis is recent exposure to nitrous oxide and elevated methylmalonic acid and homocysteine, which we can see in these patients. And treatment is rapid repletion of B12.
About the Lecture
The lecture Toxic and Metabolic Causes of Myelopathy by Roy Strowd, MD is from the course Diseases of the Spinal Cord.
Included Quiz Questions
Which of the following can cause vitamin B12 deficiency?
- Atrophic gastritis
- Duodenal ulcers
- Alcohol use
- Lack of sunlight
- NSAID use
Which of the following toxicities can cause copper deficiency?
- Zinc
- Magnesium
- Vitamin B12
- Calcium
- Vitamin D
What cause of metabolic myelopathy presents with ptosis, pigmentary retinopathy, or ophthalmoplegia?
- Vitamin E deficiency
- Vitamin C toxicity
- Copper deficiency
- Vitamin K toxicity
- Vitamin B12 deficiency
Author of lecture Toxic and Metabolic Causes of Myelopathy

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
