Playlist
Show Playlist
Hide Playlist
Sideroblastic Anemia: Etiology, Pathogenesis and Iron Studies

-
Slides Sideroblastic Anemia.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
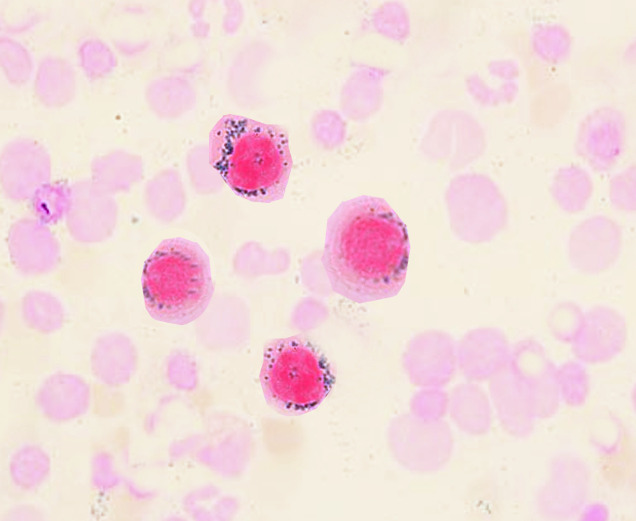
00:01 Sideroblastic Alcohol Most common? Alcohol poison resulting sideroblastic. 00:06 Another cause Lead. 00:08 Not only would lead inhibit that enzyme called, what? D, dehydrase or dehydratase. 00:16 But then also on the other side, meaning as you're getting near to producing your heme, you're also going to then inhibit ferrochelatase. 00:25 Knocking out those two enzymes. 00:27 How in the world are you supposed to form heme? You're not? And what about this child? Oh, abdominal pain? Sure, maybe lead, encephalopathy, not doing very well in school, low IQ, the lead might then actually accumulate in your epiphyseal growth plate. 00:43 And so therefore, there's a lack of endochondral ossification, the child is not going to grow very tall, so there'll be short stature. 00:50 In addition, at some point in time later on in life, there might be a lead type neuropathies And last, I told you about something like lead nephropathy. 00:59 Keep that in mind, from head to toe. 01:01 And the other thing that we'll take a look at later is basophilic stippling. 01:05 And what that basically means is there's going to be accumulation of these ribosomes and RNA particles, and such in your cells because of poisoning of these enzymes. 01:16 Next, what if your patient was taken INH without the B6 may result in lack of activity, of what enzyme? Good. ALA synthase. 01:26 Do not forget the another name for B6 is Pyridoxine. 01:29 Also keep in mind, B6 deficiency, ladies and gentlemen, could also result in peripheral neuropathy. 01:35 And do not forget, I wish to introduce this to you. 01:40 And when we talk about WBC pathology, I'll be going into myelodysplastic syndrome in much greater detail, and talk to you about a subtype or it's called Refractory Anemia of Ringed Sideroblast. 01:51 Four major different causes of more or less acquired type of sideroblastic anemia If there's a deficiency of that enzyme, you then call that your excellent recessive ALA-synthase deficiency. 02:05 Each of these inhibit different parts of the mitochondria heme synthesis, that we talked about five different mechanisms in that previous picture. 02:13 And to make sure that we are clear about what your iron studies would be here, let's quickly walk through this now. 02:20 Hemochromatosis can also be put in your only because of its iron overload. 02:25 If anything, there's too much iron. 02:28 So there might be increase serum iron, number one. 02:30 Number two, there might be too much ferritin because of too much iron here. 02:34 Number two, there is absolutely nothing blocking the release of iron by ferritin, by the way. 02:41 Well, let's just go make sure we go order every single time you go in this order, you won't be confused. 02:47 Serum iron, increased. 02:48 Number two, increased ferritin. 02:50 And number three, what kind of relationship with TIBC? Inverse. 02:54 Number three, decrease TIBC. 02:56 I told you, nothing blocking. 02:58 Nothing blocking the release of iron from your ferritin. 03:02 Therefore, what's my transferrin saturation? Increase. 03:05 It's the first one that we've seen where transferrin saturation percentage is increased. 03:11 What about iron deficiency? Oh yeah, it was decreased. 03:14 Number two, anemia of chronic disease. 03:16 Oh yeah, it was decreased. 03:18 Totally different reasons though. 03:20 In anemia, chronic disease, what happened? Remember the block? That was subsidon. Keep that in mind. 03:25 Move on. 03:31 Signs and symptoms anemia, what's that mean to you? Fatigue and tiredness. 03:35 Lab findings: We went through the increase, decrease the TIBC, and ringed sideroblasts. 03:42 What does that mean to you? Remember, the iron doesn't know where to go, it cannot couple with the heme. 03:49 So, therefore, the iron is then going to form a ring around the nucleated type of RBC and that is then called, ladies and gentlemen, ringed sideroblasts. 04:00 Bone marrow Bone marrow is where we are. 04:02 Take a look at the picture of the bone marrow where we see around your nucleus, a bunch of pressure and blue stain, Iron Welcome to Ringed Sideroblasts. 04:15 Serum iron most likely elevated decreased serum TIBC. 04:19 And then once again, do not forget that your transferrin saturation is increased. 04:24 We talked about the most common acquired cause, in fact is alcohol. 04:28 Do not forget about lead and Pyridoxine and also your... 04:34 mild dysplastic syndrome. 04:37 Ringed Sideroblast what we're seeing here with an iron stain in your bone marrow. 04:40 And the B6... 04:43 do not confuse it as a B12. 04:45 The B6 is a vitamin that's required as a co-factor with INH If the B6 isn't there, ALA-synthase isn't working properly and do not forget that B6 may also cause peripheral neuropathy. 04:59 And do not confuse this with Lead poisoning. 05:02 Lead Poisoning could also present neuropathy but totally different. 05:05 Totally different history. 05:06 There is a tuberculosis with lead, that just affect that, as I was talking about earlier, paint and such old buildings. 05:14 Abdominal pain is huge. 05:17 Keep that in mind, especially children. 05:19 And you do an abdominal imaging or X-ray. 05:22 Wow, you find opacities with that type of history... 05:25 Talk about lead encephalopathy, growth retardation, learning disabilities, peripheral neuropathy in adults and also lead nephropathy.
About the Lecture
The lecture Sideroblastic Anemia: Etiology, Pathogenesis and Iron Studies by Carlo Raj, MD is from the course Microcytic Anemia – Red Blood Cell Pathology (RBC).
Included Quiz Questions
Which of the following is a common reversible etiology of acquired sideroblastic anemia?
- Alcohol
- Myelodysplastic syndromes
- Iron deficiency
- Myeloproliferative neoplasms
- Lead poisoning
Which of the following is NOT a likely etiology for sideroblastic anemia?
- Iron deficiency
- Alcohol abuse
- Isoniazid toxicity
- Myelodysplastic syndrome
- Lead poisoning
Which of the following RBC inclusion bodies is most commonly observed in sideroblastic anemia?
- Basophilic stippling
- Howell–Jolly bodies
- Hemoglobin Barts inclusion bodies
- Hemoglobin H inclusion bodies
- Heinz bodies
Which of the following sets of serum iron study findings most likely indicates sideroblastic anemia?
- Elevated iron, elevated ferritin, elevated transferrin saturation, decreased TIBC
- Decreased iron, elevated ferritin;, elevated transferrin, decreased TIBC
- Elevated iron, elevated ferritin, elevated transferrin saturation, elevated TIBC
- Decreased iron, decreased ferritin;, elevated transferrin saturation, elevated TIBC
- Elevated iron, decreased ferritin, decreased transferrin saturation, elevated TIBC
Author of lecture Sideroblastic Anemia: Etiology, Pathogenesis and Iron Studies

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
