Playlist
Show Playlist
Hide Playlist
Sickle Cell Anemia: Pathogenesis

-
Slides Sickle Cell.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
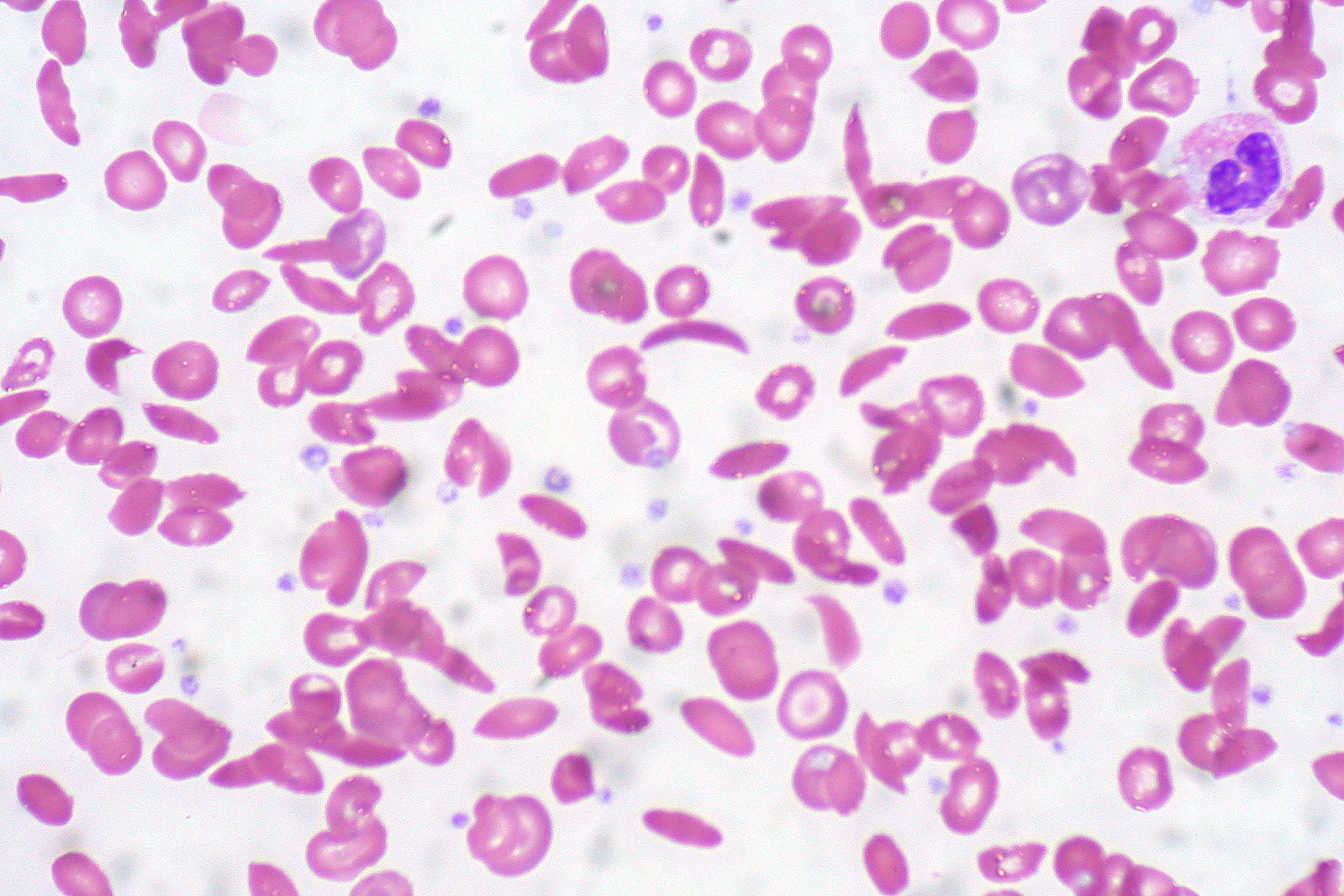
00:00 When is it that the RBC then become sickled? And what does it mean or what is the term to know as being sickling? Well, it's the fact that now you have increased demand. 00:14 So for example think about an African child who is now running. 00:19 And you should know that sickle cell disease very much runs in the African population. 00:26 So here you find a substitution that's taking place and with increased activity in a child all of a sudden that child is now suffering pain. 00:35 And we'll talk about that presentation soon enough. 00:38 Now during this episode of increased activity where the child is feeling pain, the RBCs then become sickled. 00:44 And this is called, and please know the term, polymerized. 00:48 So when an RBC gets polymerized, it means that it then looks like a sickle. 00:53 And I'll show you a picture coming up. What does this behave like? Well, I want you to think of, let's say the digits in the hands specifically. 01:01 And, let's say that you have an artery coming through. 01:03 And then, what is it gonna do? It'll bifurcate. 01:06 It will divide, divide, divide, divide into numerous divisions. 01:10 Now, say that an RBC is traveling through a big artery, and I'm gonna exaggerate here. 01:14 Plenty of room for this RBC to pass through this artery. Right? Now, you know there's increased activity and the RBC become sickled. 01:24 As you bifurcate, what happens to that diameter of your blood vessel? It becomes smaller. So now you're sickling and a bunch of RBCs that are sickled or polymerized end up at the bifurcation, at the division. 01:39 Oh my goodness. I can't move any further. What can't move any further? Blood. RBCs cannot move beyond the bunch of sickled cells that are not congregated at the bifurcation, blocking the way of getting blood into my digits. So how is the patient going to feel? Ouch. My hand hurts. Which is called clinically in sickle cell disease? Good. Dactylitis. 02:05 This is really generally speaking from head to toe known as your vaso-occlusive crisis that you find with sickle cell disease. 02:14 This is then causing the pain. Why? A decreased oxygenation to the various tissues, various meninges, what I said. 02:23 The polymerization causes sickling of the RBC under conditions of low oxygen tension. 02:28 What are these events? What are these environments? The most common being infection. 02:36 So now, you give me two differentials in which infection is now creating a anemic type of environment. 02:43 We talked about G6PD deficiency with infection and how free radicals and RBCs can't protect itself. 02:52 Here, with infection, your patient has a genetic mutation and infection is then going to bring about polymerization of your RBC. 03:00 Dehydration is another source or cause of stress, hypoxia obviously, stress. 03:09 These are conditions in which -- well, the RBC then becomes sickled, low oxygen tension. 03:15 Let's take a look at the bifurcation, what we had just discussed. 03:19 And the picture on top is showing you normal RBCs that are then moving through the bifurcation. No problem. 03:27 The picture on the bottom, you'll notice that RBCs have now become sickled. 03:31 Let's go ahead and call this the digits. 03:34 So if you go to the far right and you were to continue, let's call this a hand and you'll notice the bottom picture, there is a group or a gang of sickled RBCs that don't wanna move any further, you're blocking the way. Kinda like a thrombus, isn't it? So then what we'll do is later on, we'll further go into what's known as your vaso-occlusive crisis. 03:54 So now that you have an RBC that's sickled, well, this is -- remember, this is part of the menu for the splenic macrophage. 04:02 And so therefore you have a splenic macrophage that says, "That's sickled. Looks really good on the menu. I'll take that." Welcome to extravascular hemolysis. 04:12 In fact there might be so much extravascular hemolysis in the spleen that -- what then happens to the spleen? Splenomegaly. 04:20 What are you worried about? Autosplenectomy. What's that mean? The spleen is gonna pop out -- no. It's not gonna pop out of your stomach. 04:26 But, this spleen is then going to be destroyed and then as soon as that happens, you're thinking about your encapsuled organism and you should be thinking about vaccinating your patient with Pneumovax. 04:38 What is this called when you have such blockages you see? It's called vaso-occlusive crisis. 04:45 Allow the name to speak to you. How is the patient going to feel with a vaso-occlusive crisis? Pain. Dactylitis, acute chest syndrome. What's that mean? The blood vessels to the tissue in the lungs and such, it's not working, not functioning. 05:02 So acute chest syndrome. What else may happen? Well, the patient may then have priapism because of, once again thrombosis. 05:09 Also, you might have blockage up in the carotid so there might be, wow, stroke like issues. 05:15 Are you with me? Okay? That's your real full picture of your pathogenesis and clinical picture. 05:21 The picture here that you're seeing on peripheral blood smear, I don't want you to focus on the target cells. You do have them here. 05:28 But what you're really focusing upon here will be the sickle cell. 05:33 Take a look at that RBC, completely misshapen. 05:35 Tell me about hemolysis. Where is this? To the spleen. 05:38 How would you know that the spleen was being damaged histologically? You tell me a histologic pattern that you have been accustomed to that you've seen in medical school in which -- well, this would indicate that the spleen is being involved. 05:54 It's called a Howell-Jolly bodies. Right? These are Howell-Jolly body. 05:58 You don't see them here but this would then be an inclusion that you'd find in your RBC which to you means, "Oh, the spleen is definitely involved." And so you wanna be very careful because you're worried about autosplenectomy.
About the Lecture
The lecture Sickle Cell Anemia: Pathogenesis by Carlo Raj, MD is from the course Hemolytic Anemia – Red Blood Cell Pathology (RBC).
Included Quiz Questions
Which of the following actions or conditions DOES NOT predispose HbS to polymerize?
- Hyperventilation
- Infection
- Dehydration
- Hypoxia
- Respiratory failure
The presence of small, round, basophilic inclusions in the erythrocytes of a patient with sickle cell anemia indicates...?
- ...a nonfunctional spleen.
- ...sickle cell crisis.
- ...active hemolysis with hyperactive bone marrow.
- ...active vaso-occlusion.
- ...dysfunctional erythrocytes.
Which of the following is NOT a sign or symptom of a vaso-occlusive crisis?
- Lymphopenia
- Autosplenectomy
- Dactylitis
- Priapism
- Acute chest syndrome
Which of the following conditions is LEAST likely to cause a low oxygen tension environment for red blood cells?
- Lipoma
- Hyaline membrane disease
- Infection
- Pulmonary fibrosis
- Pulmonary edema
Author of lecture Sickle Cell Anemia: Pathogenesis

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
