Playlist
Show Playlist
Hide Playlist
Separation of Cloaca Into Urogenital Sinus and Rectum

-
Slides 07-46 Separation of the cloaca into urogenital sinus and rectum.pdf
-
Reference List Embryology.pdf
-
Download Lecture Overview
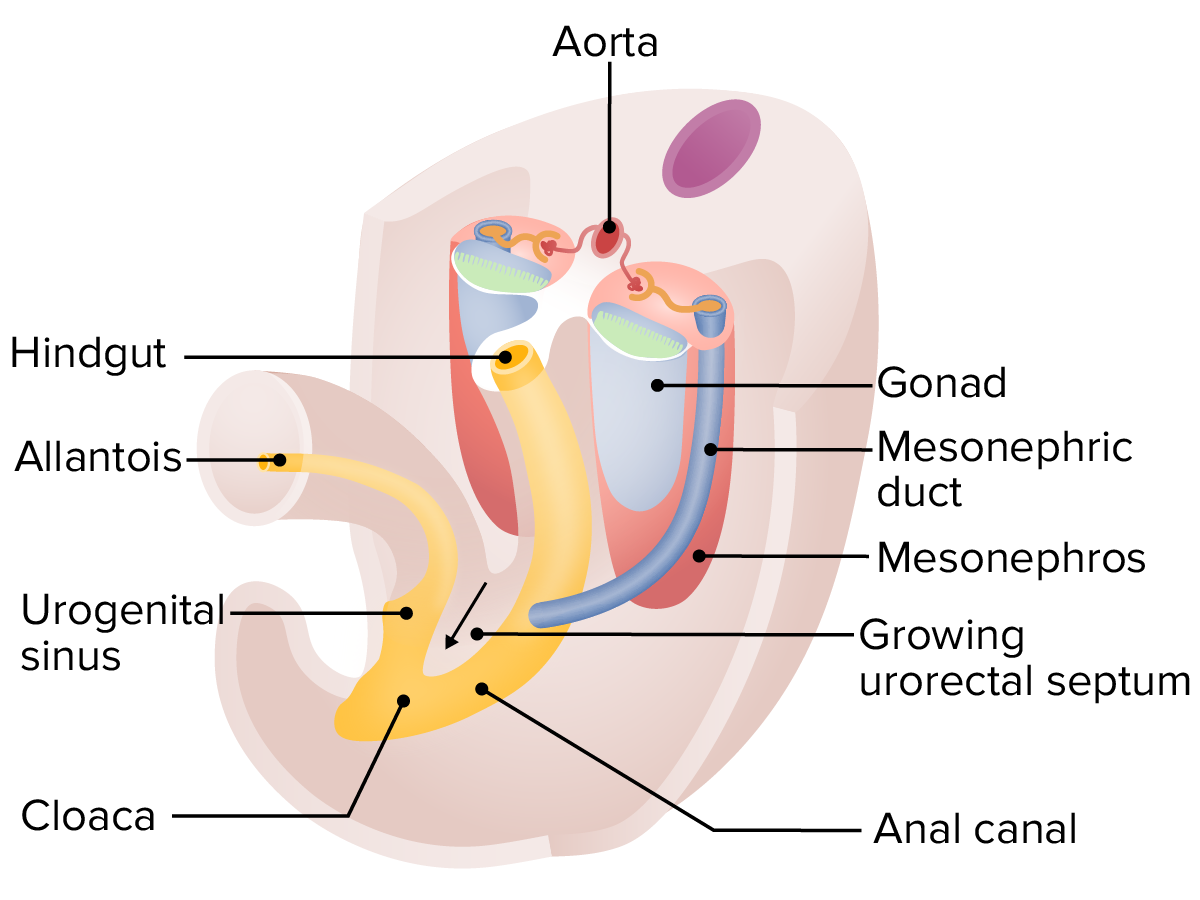
00:01 Welcome to our last lecture on development of the gastrointestinal system. 00:05 Specifically, we’re going to look at the hindgut and how it forms from a common structure called the cloaca. 00:11 The hindgut is basically the remaining portion of the gastrointestinal tract and its development is gonna be intimately tied with development of the urogenital system and we’ll discuss that specifically in another set of talks. 00:25 The hindgut is gonna be the continuation of the gut tube and it’s gonna comprise the descending colon, sigmoid colon, and rectum, and they’re all supplied blood by the inferior mesenteric artery, the last unpaired branch coming off the aorta in the abdominal cavity. 00:43 Initially, we have a common chamber receiving all the products of the urinary, the genital, and the gastrointestinal system and this is called the cloaca. 00:53 It’s a normal feature for several animals but in our case, we want to subdivide it and separate those systems a bit. 01:00 And the cloacal membrane is gonna be the only mark we see of it on the surface. 01:05 So it’s not in contact with the outside cavity yet but sooner or later, we will have rupture of that membrane and its derivatives allowing movement of fluid and food through the gastrointestinal tract. 01:18 The cloaca is subdivided into an anterior and posterior chamber by a wall of mesoderm that comes down and pushes the two away from each other. 01:27 This is called the urorectal septum and it appears in most pictures as though that septum is pushing its way straight down the midline. 01:35 In reality, the left and right mesoderm are pinching together progressively more inferiorly creating that urorectal septum and separating the cloaca into two separate components. 01:46 You’ll note we have initially a single cloacal membrane covering the cloaca but as the separation continues, the urorectal septum is going to push the two portions away from each other creating the urogenital sinus in the front, that’s going to be where the urinary and reproductive tracts will thereafter be emptying and the rectum posteriorly which is simply the end of the gastrointestinal tract lined by the endoderm that developed off the initial early gut tube. 02:15 The perineal body is a connective tissue structure that we can see on the surface from where that urorectal septum grew out and finally met the body wall. 02:24 And in the process, it’s subdivided that cloacal membrane into an anal membrane posteriorly and a urogenital membrane anteriorly. 02:34 These membranes are intact and do not actually rupture until a little further on in development. 02:40 The anal membrane, it would make sense if it simply ruptured and that was the emptying of the gastrointestinal tract but what happens is actually a bit more complex. 02:49 The rectum meets the anal membrane and is sealed off by it. 02:53 The skin on the underside of it actually invaginates and moves into the body forming what’s called an anal pit. 03:01 And the anal pit meets the rectum at the anal membrane and the line marking where those two systems come together is called the pectinate line and it’s within the anal canal and it actually marks where the skin moved in to form the anus and the rectum came down to meet it. 03:18 And that pectinate line also marks a distinct series of structures within. 03:23 There’s separate blood supply to each area and there’s separate blood drainage from each area. 03:29 So the divisions between anus and rectum is actually more significant than it might appear where we have blood drainage of the rectum drain into the portal system, to the liver, and below, branches of the internal iliac vein pull blood away from the anus. 03:46 And if we have backup of blood in any of those systems, we can develop hemorrhoids or other problems related to that region. 03:53 Now, problems that can occur in this process is that we can have the anal pit form, we can have the rectum mitted, but we can have the anal membrane fail to rupture. 04:04 This is known as an imperforate anus and essentially, our gastrointestinal system is unable to expel any fecal material out of the body. 04:13 This does have to be corrected surgically, otherwise, the affected infant will eventually die because there can be no movement of fecal material out of the body. 04:22 Similar but more severe is what’s called anal atresia. 04:26 Failure of the anal pit to form at all. 04:28 So there’s simply a smooth covering. 04:30 This also has to be corrected surgically but because there’s no anus moving in, and therefore, no muscular sphincters surrounding it to control the release of fecal material, the surgery’s a bit more complex and has to be done in multiple stages. 04:44 This is a picture of an infant who was born and we can see that there is actual anal atresia where no anus is present. 04:51 If an imperforated anus is present, the anus may appear normal but that membrane will not allow fecal material to pass through. 04:58 Hence, the importance of a good, well baby exam right after delivery. 05:02 So malformations associated with this urorectal septum moving down and subdividing the cloaca into the urogenital sinus and the rectum can be very interesting and thankfully, have a very well described nomenclature. 05:19 If we have a connection of the rectum to the vagina instead of to the anus, we have what’s called a rectovaginal fistula and this presents exactly the way you think it would. 05:32 That there will be fecal material draining into the vagina and released from there. 05:36 This obviously can happen only in women because men do not have a vagina. 05:40 Also, women could have what’s known as a persistent cloaca. 05:44 While this is very rare, it is a common chamber receiving both the urogenital sinus and therefore, the urinary and reproductive tracts, and the rectum, and once again, has to be repaired surgically. 05:56 In males where there’s no intervening uterus and vagina, a similar set of fistulas can occur where the rectum instead of connecting to the anus, connects to the urinary bladder. 06:08 That would be a rectovesical fistula and if we have that same inappropriate connection a little further down, we can have a rectourethral fistula and if you use your imagination, I’m sure you don’t want to but if you do, you can imagine exactly how these are going to pronounce, are going to present in a child. 06:31 You will have leakage of rectal material, a.k.a. feces from the urethra of the penis. 06:38 Alright, last but not least, we have a series of problems related to the innervation of the hindgut. 06:47 The neural crest cells that migrate into all regions of the gut are going to form the nerve cell plexi that continuously allow peristalsis to occur. 06:57 So as food and fecal materials move through the intestines, it’s because peristalsis and coordinated peristaltic movements from these nerve cells cause it to happen. 07:07 If the neural crest cells fail to migrate into the hindgut during weeks five to seven, we can wind up with an area that is deprived of its nerve supply. 07:16 And failure of that migration to occur is gonna cause congenital megacolon, also known as Hirschsprung's megacolon. 07:23 It is the most common form of colonic obstruction in newborns. 07:26 It happens once in every 5.000 births or so. 07:30 If there’s no ganglion cells within the smooth muscle of the gut, specifically, the hindgut, the muscle there really doesn’t know how to do anything else but contract and the affected area will be very tightly contracted causing backup of fecal material into the intestines and severe expansion of it. 07:50 Hence the name, megacolon. 07:53 So the normal colon that’s proximal to the denervated region will expand tremendously and bowel movements may be very limited, very small, and very infrequent. 08:02 A famous case of congenital megacolon is demonstrated in Philadelphia’s Mütter Museum and the affected person was said to have a bowel movement once every month and his colon was roughly the size of a tuba. 08:15 So very severe, needs to be corrected surgically, and hopefully, caught much earlier than it was in that particular individual. 08:22 Thank you very much for you attention and I’ll see you at our next talk.
About the Lecture
The lecture Separation of Cloaca Into Urogenital Sinus and Rectum by Peter Ward, PhD is from the course Development of the Abdominopelvic Region. It contains the following chapters:
- Separation of the Cloaca into the Urogenital Sinus and the Rectum
- Problems in the Hindgut Development
Included Quiz Questions
Which of the following structures arise from the hindgut?
- Distal one-third of the transverse colon, descending colon, sigmoid colon, rectum
- Proximal transverse colon, distal transverse colon, descending colon, sigmoid colon
- Ascending colon, transverse colon, descending colon
- Rectum, ascending colon, descending colon
- Cecum, ascending colon, transverse colon
Which of the following is false regarding anal development and the pectinate line?
- The pectinate line is formed by an outpouching of the rectal pit.
- Portal system drains blood above the pectinate line.
- Vena cava system drains blood below the pectinate line.
- Below the pectinate line, there is ectoderm of the anus.
- Above the pectinate line, there is endoderm of the rectum.
Which of the following is the last unpaired arterial branch to come off of the abdominal aorta?
- Inferior mesenteric
- Superior mesenteric
- Renal
- Splanchnic
- Hepatic
The cloaca is divided into an anterior and a posterior chamber; which of the following divides these two sides of the cloaca?
- A wall of mesoderm called the urorectal septum
- A wall of endoderm, called the urorectal septum
- A wall of ectoderm, called the urorectal septum
- The vitelline sheath
- The allantois sheath
Which of the following best describes imperforate anus?
- When the anal membrane remains intact
- When the anal pit does not form or meet the rectum
- When the anus does not form with muscular sphincters to control the release of fecal material
- When there is a connection between the rectum and vagina or rectal and bladder
- Failure of the neural crest cells to migrate into the gut tube
Which of the following is false regarding congenital megacolon?
- Typically it resolves without surgical intervention.
- The colon proximal to the affected segment will expand as it fills with feces.
- It results from failure of the neural crest cells to migrate into the affected region of the gut tube.
- It is the most common cause of colon obstruction in newborns.
- The lack of ganglion cells in the affected segment leads to persistent contraction of muscle, preventing movement of fecal material.
Author of lecture Separation of Cloaca Into Urogenital Sinus and Rectum

Peter Ward, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Useful lecture especially for the description of the congenital abnormalities of the developing hindgut
