Playlist
Show Playlist
Hide Playlist
Prader–Willi (PWS) and Angelman Syndrome (AS, Happy Puppet Syndrome) in Children

-
Slides PraderWilliandAngelman Pediatrics.pdf
-
Download Lecture Overview
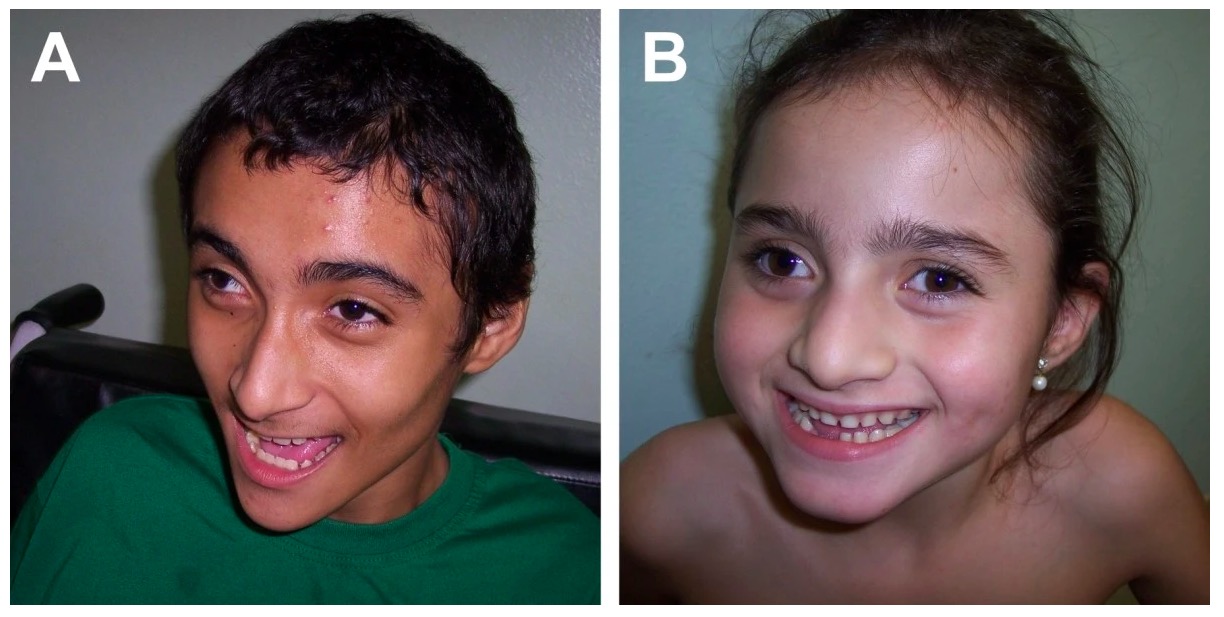
00:01 In this lecture, we will discuss the Prader-Willli Syndrome and the Angelman Syndrome. 00:06 These are interesting syndromes cause they're resulting from the same gene defect and yet present very differently based on which parent's children inherent the gene from. 00:18 So this is a result of Genomic Imprinting. 00:22 Basically, imprinted genes are genes whose expression is determined by the contributing parent. 00:29 Basically, patients only inherit 1 expressed copy. 00:34 Epigenetically, the other one is silent since one copy is silenced through methylation. 00:41 So, in this particular problem, if a father has a child, that father is going to be generally shutting down their Angelman gene. 00:51 Now, the mother has a mutation and they have a child, the child will inherit an Angelman Syndrome because the mother has mutation in the gene and the dad's is silent. 01:02 Flipside, mothers typically inactivate the Prader-Willi gene, so if the dad has a mutation, that child will now have a silent copy from the mom and will inherit Prader-Willi Syndrome. 01:15 So a way to remember this is that Prader Willi is P as paternal and Angelman Syndrome as an ANGELic mother, you can think of the mother as Angelman's. 01:29 Father mutations result in Prader-Willi and mother mutations result in Angelman Syndrome. 01:36 So what is this gene? On chromosome 15 is the SNRPN gene which is expressed only on paternally inherited copies and the E6-AP ubiquitin protein ligase gene which is expressed on maternally inherited copies. 01:53 You don't need to remember the names of these genes. 01:55 You should remember that its imprintation and which gender passes on which problem. 02:01 So with paternal, deletions result in Prader-Willi and in maternal results in Angelman Syndrome. 02:08 Enough about the genetics, let's talk about the diseases. 02:11 So Prader-Willi Syndrome typically presents with neonatal hypotonia. 02:17 These babies are born very floppy and interestingly, they have feeding difficulties, so in the first year, they can be very small and have problems with failure to thrive. 02:30 The reason why I am emphasizing this and this is somewhat ironic is that after a year of age, their muscle tone improves and they become hyperphagic. 02:41 They have this passionate need to eat and eat and eat and as a result they always almost end up being morbidly obese. 02:49 So, you wouldn't think of it but they start off as being failure to thrive in the first year and end up with dramatic weight gain. 02:56 They also have cognitive delay. 02:59 These patients also have GU abnormalities such as undescended testes. 03:05 In late toddlerhood, they start to begin to have behavioral problems that appear. 03:11 They also can have short stature and they have small hands and feet as you can see in this picture. 03:17 So this disease is very much contrasted with Angelman Syndrome. 03:22 Patients with Angelman Syndrome have severe intellectual disability. 03:26 They may have paroxysms of laughter for no particular reason. 03:30 They can have feeding difficulties. 03:32 They can have seizures and they often have a protuding jaw which is sort of a distinctive quality. 03:38 They do have a small head size. They can have scoliosis. 03:43 They may have short stature because of the difficulty of gaining weight and they tend to have somewhat ataxic gait. 03:50 So if you want to test for these patients, we will generally do a DNA Methylation Analysis where we look for what's normal and we look for whether there are equal copies of say the Prader-Willi or the Angelman and this will tell us the diagnosis. 04:06 The treatment of the Prader-Willi Syndrome is generally as much as possible diet modification. 04:13 It's really the obesity that's one of the biggest problems. 04:15 We also will engage in behavioral therapy. 04:19 We'll try to get them to change their behaviors and work with them constructively around a lot of their behavioral problems. 04:27 Oftentimes for those who have obsessive compulsive behaviors, SSRIs are benefitial in terms of limiting those behaviors and we may give them growth hormone therapy, the problem is growth hormone therapy is also associated with tonsil hypertrophy which can result in actually demise early. 04:48 So, most people steer away from growth hormone therapy unless it's absolutely needed. 04:52 The treatment of Angelman Syndrome requires an EEG and analysis and treatment of their seizure disorder. 04:59 We generally give them physical and speech therapy to try and to improve their function especially with the ataxia and we'll provide them with special education and individualized learning plans so we can maximize their potential. 05:12 So that's my review of Angelman Syndrome and Prader-Willi Syndrome. 05:17 Thanks for your time.
About the Lecture
The lecture Prader–Willi (PWS) and Angelman Syndrome (AS, Happy Puppet Syndrome) in Children by Brian Alverson, MD is from the course Pediatric Genetics.
Included Quiz Questions
Which of the following is typical in infants with Prader-Willi syndrome during the first year of life?
- Failure to thrive
- Obesity
- Hypercalcemia
- Rocker bottom feet
- Hypertonia
Which of the following is true regarding Prader-Willi syndrome?
- A deletion in the paternal chromosome 15 is the cause.
- Duplication in the paternal chromosome 15 is the cause.
- Trisomy 21 is the cause.
- It causes anorexia nervosa.
- This condition is always acquired.
Which of the following correctly compares Prader-Willi syndrome (PWS) with Angelman syndrome (AS)?
- Intellectual impairment is more severe in AS.
- PWS results from maternal mutation, while AS results from paternal mutation.
- Obesity is more commonly found among patients with AS.
- PWS patients more commonly have seizures.
- Patients with PWS have a smaller head.
Which of the following is not typically part of the treatment of Angelman syndrome?
- Low calorie diet
- Physical therapy
- Speech therapy
- Special education
- Pharmacotherapy for seizures
Author of lecture Prader–Willi (PWS) and Angelman Syndrome (AS, Happy Puppet Syndrome) in Children

Brian Alverson, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
