Playlist
Show Playlist
Hide Playlist
Progressive Supranuclear Palsy, Corticobasal Degeneration and Multiple System Atrophy

-
Slides 09 Movement Disorders Neuropathology II.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
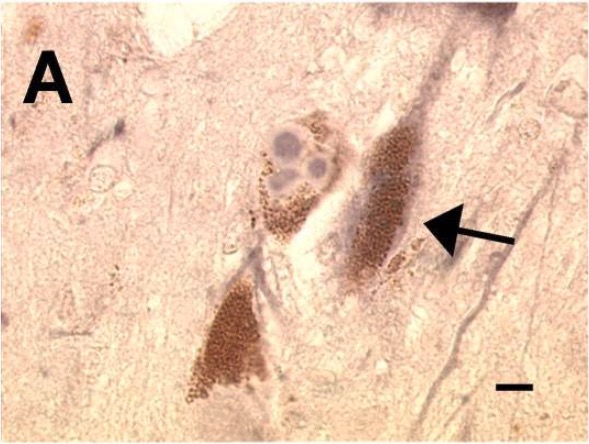
00:02 Our topic now brings us to progressive supranuclear palsy. 00:06 Progressive supranuclear palsy characterized by truncal rigidity and disequilibrium. 00:13 There will be nuchal dystonia. 00:14 What does dystonia mean? Contraction of muscle that’s taking place for long period of time. 00:19 Pseudobulbar palsy and abnormal speech, ocular disturbance, and here, it’s vertical gaze palsy, which is extremely important, and mild progressive dementia. 00:30 The clinical pearl here is going to be vertical gaze palsy. 00:33 Progressive supranuclear palsy. 00:37 Its onset is between the fifth and seventh decades of life and studies have shown that males and females could share equal preponderance. 00:49 The pathology: So what’s happening in progressive supranuclear palsy? Neuronal loss in the globus pallidus. 00:56 Think about that for one second. 00:58 Subthalamic nucleus, substantia nigra, colliculi, periaqueductal gray matter and dentate nucleus of the cerebellum. 01:05 There’s neural loss in many of these structures that we’ve identified here. 01:11 Neurofibrillary tangles could also be found, but remember neurofibrillary tangles is something that we find in every individual who gets older, elderly, okay? Those neurofibrillary tangles are structurally similar to what is seen in Alzheimer’s, but the chemical tau filaments are single and straight, in contrast to the typical paired helical. 01:29 However, if the patient starts showing you signs of Alzheimer’s disease, then the number of neurofibrillary tangle is going to then correlate with the severity of the disease itself. 01:41 Our topic here is corticobasal type of degeneration. 01:44 The definition. 01:46 It’s a disease of the elderly characterized by extrapyramidal rigidity. 01:51 Asymmetric motor disturbances. 01:54 In other words, a multifocal type of myoclonus and sensory cortical dysfunction. 01:59 By cortical dysfunction, you should be thinking about higher order type of activity including apraxia, disorder of language, and then here, alien hand type of phenomenon. 02:11 All of this is referred to as being your corticobasal type of degeneration. 02:16 Allow the name to speak to you. 02:17 The pathology here will be cortical atrophy of motor, premotor, or perhaps even anterior parietal lobes. 02:25 Hence, we talked about the language disorder that might be taking place, and we talked about that alien hand type of phenomenon. 02:32 Neuronal achromasia: severe loss of neuron, gliosis, and ballooned neurons. 02:39 Corticobasal, ballooned neuron. 02:41 Substantia nigra and locus ceruleus show loss of pigmented neurons and something that we refer to as being your argyrophilic type of inclusions. 02:51 Corticobasal type of degeneration. 02:54 Multiple systemic type of atrophy. 02:57 It’s a spectrum of diseases, characterized by presence of glial cytoplasmic inclusion, typically with cytoplasm of oligodendrocytes. 03:07 So here, when you think about multiple system atrophy, it’s a spectrum, and we’ll talk about this a little bit moving forward. 03:14 Clinical features: Well, here, we have something called striatonigral type of degeneration. 03:20 This as you can expect very much so will be movement disorder resistant to L-Dopa because literally, it’s a destruction or degeneration of the nigrostriatal pathway. 03:31 Atrophy of the caudate nucleus and putamen is involved. 03:35 Nuclei show extensive neuronal loss and marked gliosis. 03:39 Remember, gliosis always means your repair mechanism for the brain, doesn’t it? And when we say repair mechanism in the brain, remember that we do not have fibroblasts in the brain. 03:49 So therefore, there is no scar formation technically. 03:52 Yet, we call it a glial scar and we talked about this in general pathology that that “glial scar” is a misnomer and the fact that we do have microglia that are coming in to remove the debris, but gliosis to you should mean rather marked damage or that injury is taking place to the brain itself. 04:10 Under multiple system atrophy, we have a couple other variants that I’ll quickly walk you through. 04:18 Let’s go with Shy-Drager syndrome. 04:20 It’s an extrapyramidal syndrome that combines your autonomic system dysfunction. 04:25 So by this we mean that if you’re lying in a supine position where at this point you have increased blood flow to the heart, supine position, and then all of a sudden you go from a supine or even a sitting position to a standing up position, then you’re going to pool your blood down in the legs very quickly. 04:42 And if you have autonomic type of instability, then please understand that you’re going to exhibit what’s known as orthostatic hypotension. 04:50 Impotence, your sweat glands and, in general, your glands are not working properly and papillary abnormalities. 04:57 Parkinson. 04:59 Another type of multiple system atrophy, with something called olivopontocerebellar atrophy. 05:06 As the name implies, there will be cerebellar degeneration that’s taking place. 05:10 And as soon as the cerebellum is being affected, then you can expect there to be a type of ataxia. 05:17 Eye and somatic movement disorder. 05:19 Dysarthria, and then rigidity as well.
About the Lecture
The lecture Progressive Supranuclear Palsy, Corticobasal Degeneration and Multiple System Atrophy by Carlo Raj, MD is from the course Movement Disorders. It contains the following chapters:
- Progressive Supranuclear Palsy
- Corticobasal Degeneration
- Multiple System Atrophy
Included Quiz Questions
A 65-year-old man comes to the physician's office complaining of loss of balance and abnormal speech. Further history from his family reveals that he is also experiencing dementia. A physical examination shows truncal rigidity and nuchal dystonia. Which of the following is a prominent feature of his likely diagnosis?
- Vertical gaze palsy
- Horizontal gaze palsy
- Miosis
- Internuclear ophthalmoplegia
- Ptosis
A 60-year-old woman presents to the clinic with spasmodic movements in different parts of her body. A physical examination shows rigidity and she is unable to perform simple motor tasks. What is the most likely diagnosis?
- Corticobasal degeneration
- Parkinson disease
- Multiple sclerosis
- Multiple system atrophy
- Lewy body dementia
A 55-year-old Caucasian man presents to the clinic with erectile dysfunction. He also complains of dizziness while standing up from a supine position. He has a history of hypertension, type 2 diabetes mellitus, and COPD. A physical examination reveals dryness of the skin and a gait test shows loss of balance. What is the most likely diagnosis?
- Shy-Drager syndrome
- Parkinson disease
- Upper motor neuron disease
- Huntington Disease
- Progressive supranuclear palsy
A 60-year-old man with a history of diabetes, hyperthyroidism, and hyperlipidemia presents to your clinic with slurred speech. He also complains of difficulty in his vision and a loss of balance. A physical examination shows rigidity in his muscles and an inability to maintain balance. What is the most likely pathology of his condition?
- Cerebellar stroke
- Nigrostriatal pathway degeneration
- Cerebral degeneration
- Neurofibrillary tangles
- Upper motor neuron disease
Author of lecture Progressive Supranuclear Palsy, Corticobasal Degeneration and Multiple System Atrophy

Carlo Raj, MD
Customer reviews
3,5 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
1 |
| 1 Star |
|
0 |
I love your lectures. I learn so much. So good at teaching. Thanks.
Just reading the slides.No explanation.No schematic drawing to show the involved areas or the characters of the diseases.No pathological sections, gross or microscopic.
