Playlist
Show Playlist
Hide Playlist
Prader-Willi Syndrome

-
Slides 02 Chromosomal Disorders II.pdf
-
Download Lecture Overview
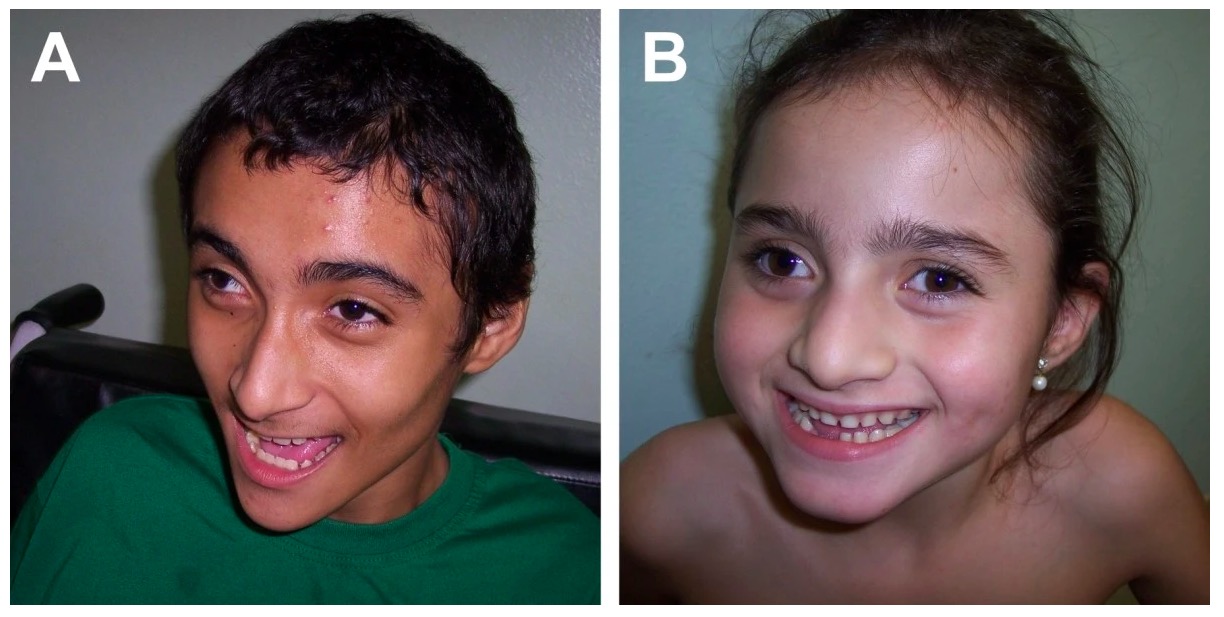
00:00 Looking at Prader-Willi syndrome specifically, hopefully, this will bring some more sense to it. 00:07 But if you get lost, go back to those intro slides because I swear, it’s all lined up perfectly. 00:12 It should be able to put you back in the right box of understanding. If I’ve done a really good job at this, you won’t be lost at all. Let’s take a look at the paternal and maternal chromosome. 00:24 They both have these regions. However, I’m going to add some highlighting here to show that the region that is Prader-Willi syndrome is imprinted or turned off, hypermethylated on the maternal chromosome, right? So, if the paternal chromosome has a deletion in that same region, this is the region that would most commonly be deleted, then there are no genes for Prader-Willi being expressed because the father, the paternal chromosome doesn’t have them because they’re deleted and the maternal chromosome, they’re turned off. So that whole region, there is no dosage of the genes associated with the Prader-Willi syndrome. Now, because none of these things are expressed, we end up with the phenotype that we do with Prader-Willi. So, no Prader-Willi syndrome genes expression, then we have Prader-Willi syndrome. Again, Prader-Willi syndrome is very different in its expression than Angelman because as you can see, they’re different genes. The major phenotypic features of Prader-Willi that you should understand, I’ll say the first thing most importantly is that Prader-Willi kids tend to be quite obese because they really have completely insatiable appetites. There’s something that’s altered in the hypothalamus as far as satiation and they just never feel satisfied. But interestingly as infants, they have feeding difficulty. So they’re not able to feed or nurse properly. It’s only when they develop into childhood, they have hyperphagia and obesity and again, super uncontrolled need to eat. 02:22 They’re always, always hungry. We also see hypotonia. The muscles again aren’t contracting at full strength, some cognitive impairment, not entirely a large amount of cognitive impairment but some cognitive impairment. They’re generally short in stature and often have smaller hands and feet. 02:42 These are just general symptoms, images of what Prader-Willi syndrome can look like. It’s important in counseling parents with Prader-Willi kids to consider or understand that they’re really never satisfied in the appetite. So, a lot of this is around having to train eating habits without being satisfied. 03:10 I think that sounds like a terrible condition.
About the Lecture
The lecture Prader-Willi Syndrome by Georgina Cornwall, PhD is from the course Chromosomal Disorders.
Included Quiz Questions
Which of the following describes the eating habits of Prader-Willi patients throughout their lifetime?
- Poor feeding in infancy and hyperphagia in childhood
- Hyperphagia in infancy and poor feeding in childhood
- Hyperphagia throughout life
- Poor feeding throughout life
- Hyperphagia in infancy and normal feeding in childhood
Which of the following is NOT a phenotypic feature of Prader-Willi syndrome?
- Cleft palate
- Cognitive impairment
- Short stature
- Small hands and feet
- Hypotonia
Author of lecture Prader-Willi Syndrome

Georgina Cornwall, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
2 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
very well done and nice explication, very good material to the step 1
Excellent ! I finally understand the topic after forgetting it many times ! Much better than First Aid !
