Playlist
Show Playlist
Hide Playlist
Pneumothorax in Radiology

-
Slides Pneumothorax.pdf
-
Download Lecture Overview
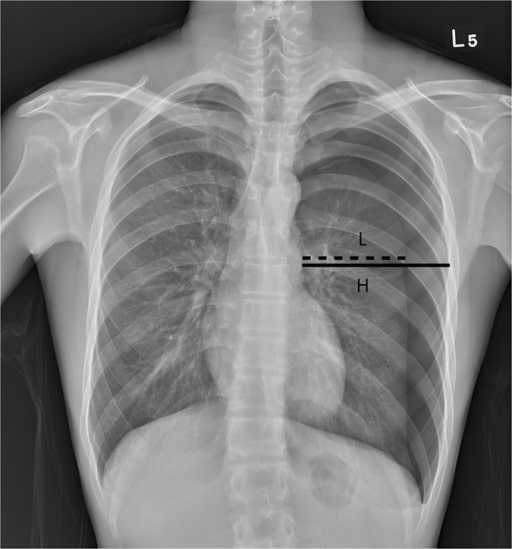
00:01 So, let's move on to pneumothorax. 00:03 This is a finding that you really don't want to miss because if it's large, it needs immediate intervention, so let's take a look at some of the imaging findings. 00:11 A pneumothorax is entrance of air into the pleural space which causes the lung to collapse, the parietal and the visceral pleura separate when this happens. 00:22 So, a pneumothorax results in a thin white line which represents the visceral pleura. 00:29 You have complete absence of lung markings peripheral to the visceral line and this is most often seen at the apex on an upright radiograph because the air rises up towards the apex. 00:39 Pneumothoraces can actually be very difficult to see and you have to train your eye to looking at these. 00:44 So let's take a look at a few examples and then feel free to pause and take a good look at these so that you can just train your eye to visualizing these. 00:52 In the supine position, air actually travels to the non-dependent portion of the lung and collects laterally and anteriorly in the pleural space. 01:02 The pneumothorax is less likely to be seen at the apex on a supine film because again, air is gravity dependent. 01:10 So this results in what's called the deep sulcus sign which is a lucency inferiorly which displaces the ipsilateral costophrenic angle and you can see that here on the left, with a large lucency in the left lower costophrenic angle. 01:27 So, how about on a CT? Air is usually seen anteriorly on a CT. 01:34 Again, because it's gravity dependent and the patient is lying supine. 01:38 A CT is actually much more sensitive, especially for the evaluation of a very small pneumothorax. 01:43 And you can see here a normal right lung and in the left you actually have multiple cavitary lesions, possibly an area of consolidation likely representing a pneumonia. 01:54 And then, a relatively large pneumothorax or absence of lung anteriorly. 01:59 Some common causes of pneumothorax include trauma which can be caused by something like a rib fracture, they can occur spontaneously, often occurring in tall thin young males. 02:11 They can be Iatrogenic which may follow as something like a lung biopsy. 02:16 They can be the result of asthma or rupture of an alveolus or a bleb, or they could be a result of COPD or cystic fibrosis, again because of rupture of an alveolus or a bleb. 02:26 Let's take a look at this patient here. 02:29 Do you see a pneumothorax on this film? So, the green lines point to the visceral pleural line. 02:42 This patient does have a pneumothorax on the right. 02:44 And how about this patient, do you see anything abnormal in this patient? Which side is the abnormality and let's start from there? Here's a more zoomed in image of the right lung. 03:00 The abnormality is on the right. 03:02 Alright, so this patient actually has a pneumothorax. 03:07 You can see the visceral line pointed out by the white arrows. 03:10 Can you tell what the cause of this pneumothorax is? So this is actually a hydropneumothorax. 03:21 So the air is pointed out by the blue arrow and there's also fluid in the pleural space which is pointed out by the white arrow. 03:28 So the pleural space can accumulate both air and fluid, a normal pleural effusion is also located within the pleural space. 03:34 When you have a combination of both air and fluid, this is called a hydropneumothorax. 03:39 In this patient, the pneumothorax is actually caused by a rib fracture which you can see by the circle and that indicates that this fluid is likely blood which you can call a hemopneumothorax. 03:51 So let's take a look at this patient here, which side is the abnormality on? So, this is an example of a tension pneumothorax, the abnormality is on the left, and you can see that there is shift of the mediastinal structures away from the side of the pneumothorax, this can actually result in hemodynamic collapse and this is one of the findings that you really don't want to miss. 04:18 This patient needs an urgent decompression with a chest tube, oftentimes, this decompression is performed right at the emergency room as soon as we've diagnosed this.
About the Lecture
The lecture Pneumothorax in Radiology by Hetal Verma, MD is from the course Thoracic Radiology. It contains the following chapters:
- Pneumothorax
- Causes of Pneumothorax
Included Quiz Questions
Which of the following is NOT associated with a pneumothorax?
- X-ray visualization of the thin white line, which is the parietal pleura
- It can be iatrogenic after a biopsy.
- Lack of lung markings in the periphery of the lungs
- The shift of the mediastinal structures is an emergency and requires urgent decompression.
- It can occur spontaneously in thin young males.
Which is the most common site on an upright radiograph for visualization of pneumothorax?
- Apex
- Perihilar
- Left lower lobe
- Right middle lobe
- Right lower lobe
Which of the following is NOT true regarding the deep sulcus sign?
- The heart displaces to the side of the sulcus.
- In the supine position, air travels to the non-dependent portion of the lung.
- In the supine position, air collects laterally and anteriorly in the pleural space.
- It is less likely to be seen at the apex on a supine film.
- It is the lucency and inferior displacement of the ipsilateral costophrenic angle.
Which among the following is NOT a common cause of pneumothorax?
- Viral bronchitis
- Asthma
- Cystic fibrosis
- Spontaneous
- Biopsy
Author of lecture Pneumothorax in Radiology

Hetal Verma, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
