Playlist
Show Playlist
Hide Playlist
Pneumothorax & Pleural Effusion: Pleural Effusion



-
Slides SpecificDiseases RespiratoryPathology V2.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
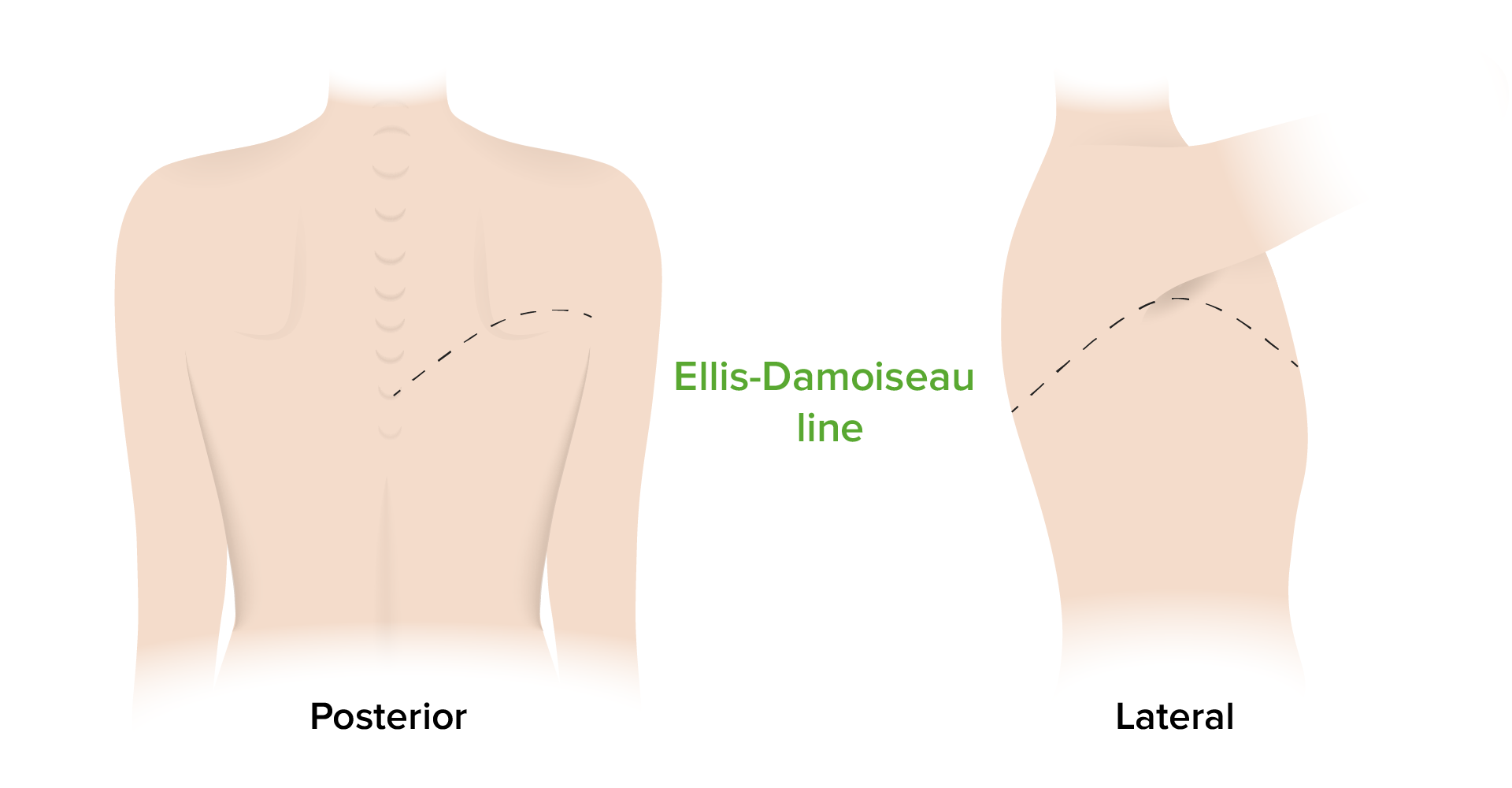
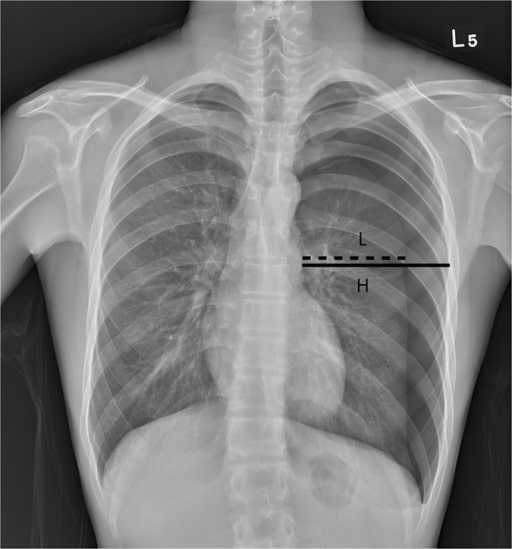
00:01 We're moving to pleural effusion and with pleural effusion this is not air in my pleural cavity, please take a look, this is fluid between the pleural layers. 00:14 What kind of fluid? Well, it depends. 00:16 Now earlier we talked about accumulation of fluid in your pericardial cavity, didn’t we? We had pericardial effusion and during that discussion we looked at cardiac tamponade being rapid accumulation of fluid in the pericardial cavity therefore causing constriction of the heart. What did you do there? You opened up that window, removed that fluid that’s called pericardiocentesis. 00:41 What's this called here, when you wish to remove fluid from the pleural cavity, it's called thoracentesis. Straight forward. 00:47 Now, something that I wish to bring to your attention is the differences on x-ray here of atelectasis and effusion. 00:57 First, let's take a look at atelectasis. 00:59 When was the last time we looked at atelectasis? We looked at atelectasis when we were talking about acute respiratory distress syndrome. 01:07 We talked about this in an adult being the most common cause such as sepsis. 01:12 What else could occur? Aspiration pneumonia, so on and so forth. 01:17 Do you remember that discussion? Good. 01:19 And then under neonatal respiratory distress syndrome, we talked about, most commonly, if surfactant is deficient, in babies born at less than 28 weeks of gestational age, it results in atelectasis. 01:31 And what you're looking at here in atelectasis, the mediastinum is pulled towards the collapsed lung side, that’s a basically think of collapsing of the alveoli and once again, for the most part, pulling the mediastinum to the side of the lesion versus effusion. 01:50 Your effusion is going to be accumulation of fluid in your pleural cavity and thus, what happens here? The effusion pushes the mediastinum away towards the contralateral side that’s what you're thinking here, just away, effusion. 02:06 And take a look at that x-ray - that is rather filled, this is not ladies and gentlemen pulmonary edema secondary to left-sided heart failure, because it was pulmonary edema you would find there to be increased opacity bibasilar and equal, not like what you're seeing here because the pleura, it surrounds the entire lung so therefore if there's pleural effusion it’s like it's covering the entire lung instead it's covered in opacity. 02:34 You see the big difference between our effusion on your right and the atelectasis on your left - in the left you don’t have such marked and homogenous type of opacity over the lung, but what it will do is pull this side of the mediastinum if it's bad enough. 02:52 Let's talk about the different types of effusion. 02:58 Just like we've done about edema, we’ll do the same thing with the effusion but we will go to a lot more detail here especially the next table where things become a lot more clinical for us. 03:08 So to begin with, quickly transudate, close your eyes. 03:12 Transudate - protein poor most likely cause, increase hydrostatic pressure pushing the fluid into the good, interstitium. 03:22 Welcome to left sided-heart failure and we've also talked about nephrotic syndrome and cirrhosis. Lack of protein, decreased oncotic pressure, nephrotic syndrome, how much, how much protein are we losing? Good, greater than three and a half grams of protein per day and cirrhosis, you're not producing albumin. 03:41 Exudate - protein rich. What's going on here? Mostly, please take a look, non-cardiac origin. 03:50 So think about, look at your differentials here - we have pneumonia, cardiovascular disease, trauma. What is happening? It's a fact that you are now causing damage to the lung, the other big one is TRALI, which is transfusion related acute lung injury, that’s a big one. 04:08 Anyhow, all of those are causing injury to the lung, acute inflammation, or what happens to capillary permeability? Good, it increases thus what are you releasing into the interstitium? Protein rich - welcome to exudate. 04:23 And then we can have lymphatic, what happens here? Well thoracic duct injury from trauma. 04:28 Malignancy is the big one, resulting in what's known as chylothorax therefore, what kind of effusion would you call this? This is going to be lipid in your pleural cavity, is that clear? So look for lymphatic issue as well, please, as far as a third and really this is the first time that I'm introducing a lymphatic type of fluid accumulation, this is chylothorax.
About the Lecture
The lecture Pneumothorax & Pleural Effusion: Pleural Effusion by Carlo Raj, MD is from the course Disorders of the Pulmonary Circulation and the Respiratory Regulation: Basic Principles with Carlo Raj.
Included Quiz Questions
Which of the following is NOT a potential etiology of exudative pleural effusions?
- Cirrhosis
- Pneumonia
- Trauma
- Malignancy
- Collagen vascular disease
What is the most common etiology of transudative pleural effusions?
- Congestive heart failure
- Superior vena cava obstruction
- Pulmonary embolism
- Thoracic duct injury
- Malignancy
What is the underlying mechanism most etiologies of exudative pleural effusions share?
- Increased capillary permeability
- Decreased vascular oncotic pressure
- None of the answers are correct
- Decreased hormonal influence on vasoconstriction
- Increased vascular hydrostatic pressure
Author of lecture Pneumothorax & Pleural Effusion: Pleural Effusion

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
