Playlist
Show Playlist
Hide Playlist
Pneumothorax & Pleural Effusion: Physical Findings of the Lung



-
Slides SpecificDiseases RespiratoryPathology V2.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
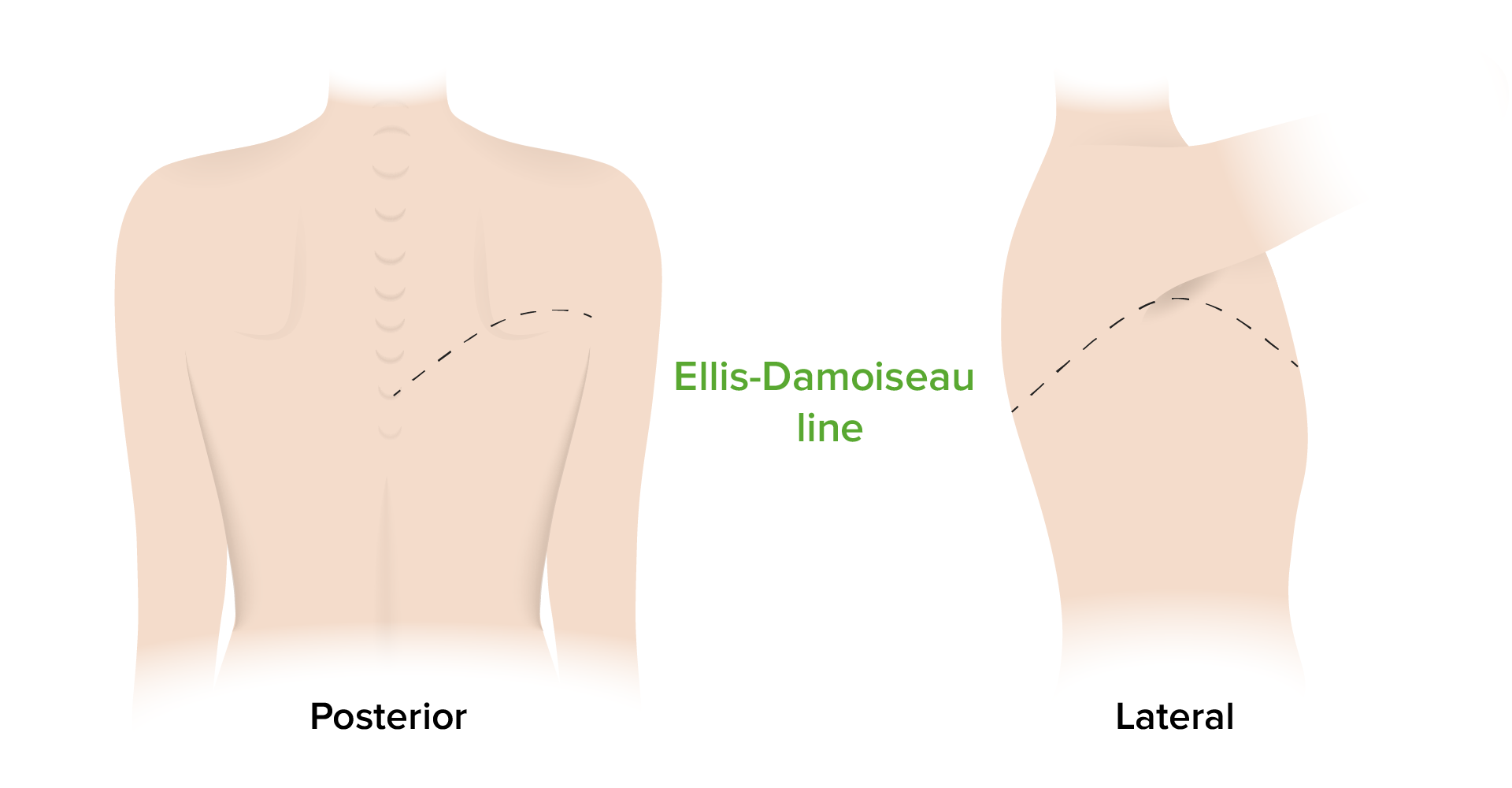
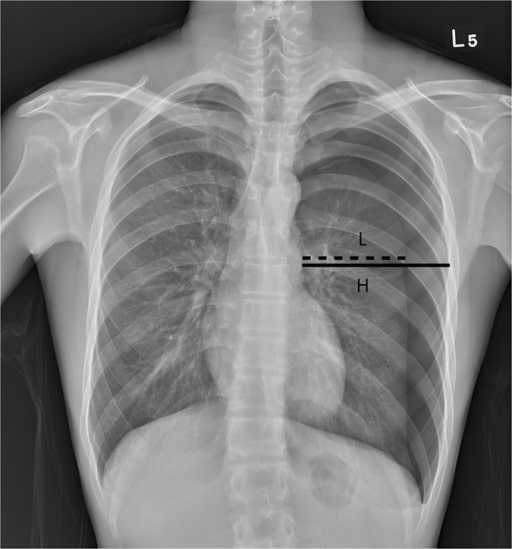
00:01 On this table, we’ll walk through the various pathologies in the first column and then we will take a look at the various clinical and physical examinations that you hopefully at some point in time have done in many of these patients and if you haven’t, then at least be able to understand what you’re expecting to hear and such. 00:23 Let’s do a pleural effusion. 00:25 First, close your eyes think about that x-ray that I just showed you it was completely filled with fluid, whatever it may be, and if that’s pleural effusion then understand that it’s covered by opacity. 00:36 So now you want to think about your lung being compressed, what do you think happens to your breath sounds? Decreased. 00:43 Now if you were to percuss, how do you do the action of percuss? Well, if your pleural cavities is field with fluid - dull. Fremitus, tactile decreased. 00:56 What about tracheal deviation? Either or not applicable or if the pleural effusion is bad enough, large, what is it going to do? Tracheal deviation away from the side of the lesion. Common sense, logic, but you need to be clear about what you're doing. 01:14 Let’s do our next one - atelectasis. Here, what then happens please? Absolute collapse of the alveoli, we’ve talked about the differentials. 01:22 Breath sounds is decreased, percussion dull, fremitus decrease, next, atelectasis - what is it going to do? It kinda behaves like your open pneumothorax, gonna pull the trachea to the side, pull the mediastinum to the side of injury. 01:38 Simple, what's happening in simple? Well, keep it simple. 01:43 It's a fact that yes, you're introducing positive pressure, excuse me - atmospheric pressure slightly into the pneumothorax, but it's still be sub-atmospheric slightly compared to the other one, but the fact that you're introducing air into the pleural cavity, breath sounds decreased, okay - you have something in your pleural cavity, however because this is hair, excuse me, air, then it will be hyper-resonance, and you get hair into your pleural cavity. 02:07 You heard it here from Dr. Raj, no, it's air, that’s what I meant to say so hyper-resonant because of air. 02:13 Fremitus is decreased, tracheal deviation it's simple - it is not severe so therefore not applicable clinically, tracheal deviation or mediastinal deviation. 02:25 Now, we’re getting to tension and open, we’ll put this together. 02:29 First tension pneumothorax, what is it doing? Ball and valve effect, you open the valve upon inspiration, upon expiration the valve closes, air gets trapped where? Good in the pleural cavity. Now, breath sounds? Decreased. 02:45 Let's do open pneumothorax. 02:48 Open pneumothorax such as a gunshot wound, open communication with the atmosphere, what then happens? Good, you have extreme positive pressure, this lung is going to collapse. 03:00 Either case, you have a decreased breath sounds, all cases here of pneumothoraxes are hyper-resonant upon percussion. 03:10 Tympanic, okay? Next, fremitus will be decreased. 03:14 Now let's talk about tracheal deviation. 03:16 Upon - let's say, close your eyes, I'm just reading this to you. 03:20 You tell me which one is which, open and tension, are you ready? Close your eyes, seriously. 03:25 Okay. Upon, exploration away from the site of injured lung, tracheal deviation. 03:30 Which one is this? Tension or open? Upon expiration away from the site of injured lung - this would mean upon expiration the valve closed tension increased, pushed the trachea mediastinum to the other side, so that was a description of tension. 03:50 Then, if it's open, upon expiration, towards the side of the injured lung - is that clear? So upon expiration, what then happens? Well, you're going to have collapse and so therefore it's gonna pull the mediastinum or trachea to the side of the injured lung - your focus upon expiration. 04:11 Let's take a look at lobar pneumonia and pulmonary edema, put those together. 04:15 Picture this, let’s say its lobar pneumonia and secondary to pneumonia, like with streptococcus pneumonia. 04:23 Pulmonary edema maybe secondary to left-sided heart failure. 04:26 First, well, what kind of sounds? Inspiratory crackles late. 04:31 Bronchial breath sounds, you should never be hearing breath sounds in the bronchi for Pete’s sakes in the proximal portion - no, no, no. 04:39 That’s the pathology. 04:40 Here percussion it’s like having a block or brick as a fluid or maybe lobar, so this is dull percussion. 04:48 Here the fremitus will be increased only one thus far in which when we find it, increase in fremitus. 04:55 Tracheal deviation, not clinically applicable here as well. 04:58 Please spend some time on this table, I would say it’s probably one of the most important tables to really bridge the gap and integrate the understanding of your pathologies and then really putting this together and connecting the bridge into your clinical picture of what you can expect with your patient, either with you doing the physical examination or which you can expect to see on your chest x-ray and such. 05:21 Let’s continue. 05:22 So you have edema, how can you tell the difference between exudate and transudate? Exudate means protein rich. What is it called when you have edema in your serosa? It is then referred to as being effusion. 05:37 So irregardless is to where the edema is located, you then have to have a particular criteria, which is then known as your Light’s Criteria rule. 05:44 In the Light's Criteria rule you just need one component for it to determine whether or not you have exudate or not. 05:52 The fact that you just require one component makes it extremely sensitive at the expense of not being too specific. 06:00 Let’s take a look at what the LCR, Light’s Criteria Rule are. 06:05 If you find pleural protein to serum protein greater than 0.5 then that would obviously refer to that Pleural Effusion being of the exudate type and if found to be less than 0.5, transudate. 06:21 We know that it’s already protein rich, exudate. If you found the pleural LDH compared to the serum LDH ratio being greater than 0.6, well, you find that, that is exudate of the pleural effusion if you find that the pleural LDH is at greater than two thirds the upper limit and the laboratories are normal serum LDH, well that will be a determinant of exudate. 06:51 Now the different type of effusion or exudates that you could have if there's high cholesterol, this then obviously refer to as chylothorax, in other words triglycerides. 07:01 Your pH tends to be low, and if you find that LDH, I'm gonna give you the rule of thumb, here, if you find that LDH to be greater than 1000 iu per liter, please know that you're in the territory of empyema. 07:17 Empyema of course referring to, my goodness, extreme, extreme bacterial infection taking place. 07:23 Here you’d expect the pH to be quite low and obviously here with exudate, if there is an inflammatory process, you can expect to find more cells.
About the Lecture
The lecture Pneumothorax & Pleural Effusion: Physical Findings of the Lung by Carlo Raj, MD is from the course Disorders of the Pulmonary Circulation and the Respiratory Regulation: Basic Principles with Carlo Raj.
Included Quiz Questions
Which of the following is a differentiating feature of pneumothorax from atelectasis, pleural effusions and lobar pneumonia?
- Hyperresonance on percussion
- Vesicular breath sounds
- Tracheal deviation
- Inspiratory crackles
- Decreased tactile fremitus
Which of the following is NOT an expected physical finding in atelectasis?
- Bronchial breath sounds
- Hypoxemia
- Tracheal deviation towards the affected side
- Decreased tactile fremitus
- Dull to percussion
Which of the following pleural fluid findings would suggest pleural effusion of cardiogenic etiology?
- Pleural protein/serum protein < 0.5
- Pleural LDH/serum LDH > 0.6
- WBC > 1000 per cubic millimeter
- pH < 7
- Pleural cholesterol > 45 mg/dL
Which of the following would you expect to be elevated in the pleural fluid of a patient with a thoracic duct injury?
- Triglycerides
- pH
- LDH
- RBCs
- WBCs
Author of lecture Pneumothorax & Pleural Effusion: Physical Findings of the Lung

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
