Playlist
Show Playlist
Hide Playlist
Partitioning and Malformations of the Urogenital Sinus

-
Slides 08-49 Development of the microscopic kidney.pdf
-
Reference List Embryology.pdf
-
Download Lecture Overview
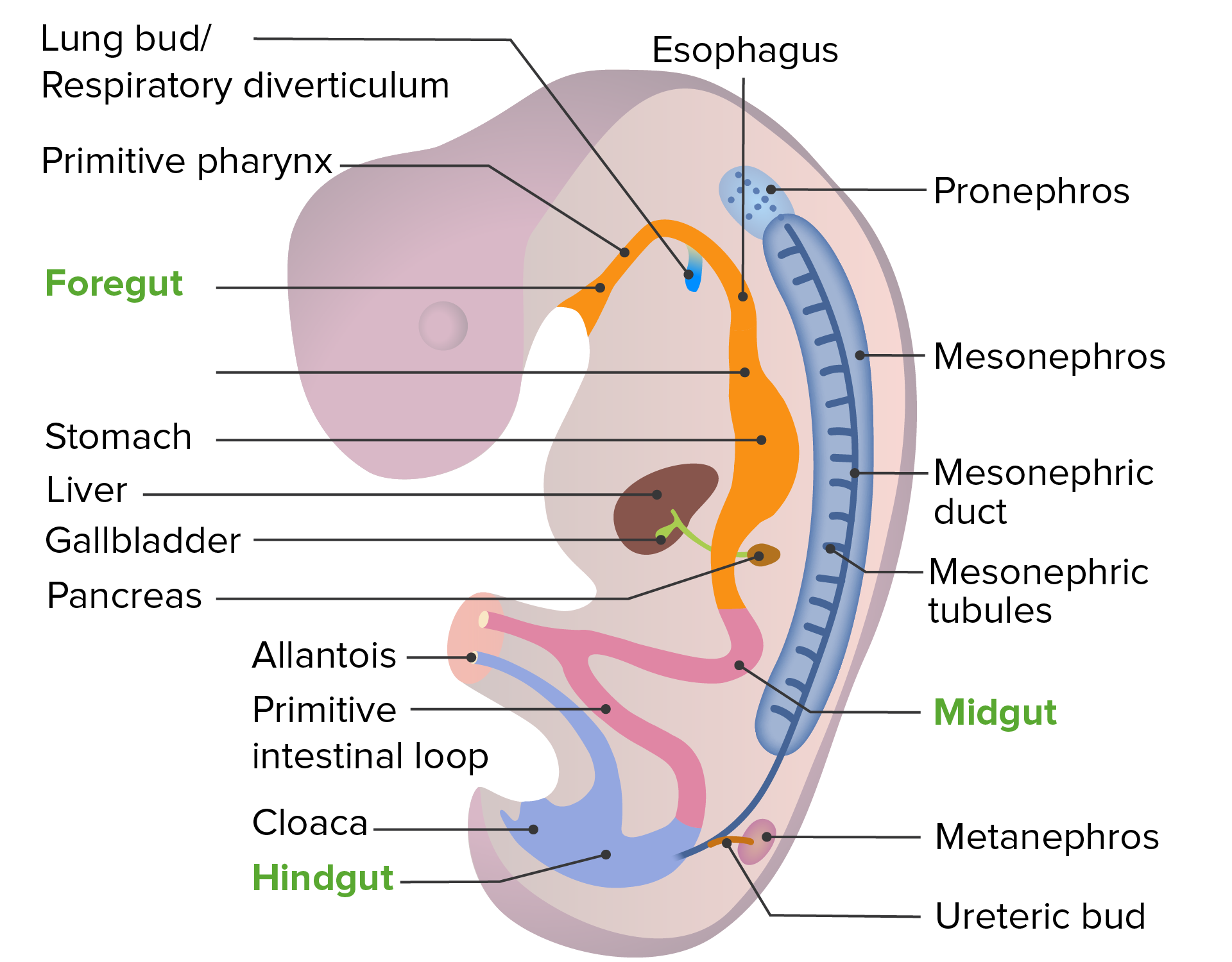
00:01 Hello, we’ll be discussing now the partitioning of the urogenital sinus and its role in renal development. 00:08 Now, last time we discussed the urogenital sinus, it was in the context of development of the hindgut. 00:15 You may recall that initially, we have a cloaca, a common chamber that drains the GI urogenital systems and it gets separated into a separate rectum and urogenital sinus as a massive mesenchyme moves down called the urorectal septum. 00:35 The urorectal septum moves down and forms a little knot of connective tissue at the base of the perineum called the perineal body. 00:43 And in the process, separates the cloaca into the rectum and the urogenital sinus. 00:48 Any you may also remember if you viewed the discussion on hindgut development that the cloacal membrane also separates into an anal membrane and a urogenital membrane. 00:59 At this point, I want to draw your attention to a thin little strip of endoderm that’s extending off the urogenital sinus up into the umbilical cord. 01:08 That is the allantois or if you prefer the proper French pronunciation, the allantois and it acts as a very, very early filtration system for the developing embryo but is otherwise not really used by the mammalian body except that it can wind up causing some developmental anomalies if it doesn’t rescind properly. 01:30 Typically, the allantois is going to dwindle, move in from the umbilical cord, and just take up residence on top of the urinary bladder, and eventually, form a fibrous cord that’s called the urachus. 01:43 So generally, it goes away, it doesn’t really leave much behind except a fibrous cord extending from the umbilicus down to the very tip of the bladder. 01:52 The urogenital sinus is thereafter gonna form the urinary bladder as well as the urethra. 01:58 In women, the urinary bladder allows urine to leave to the urethra and enter the vestibule alongside the opening of the vagina. 02:07 In men, there’s going to be some folds of tissue that surround the urethra, so these urethral folds will wrap around it and form the shaft of the penis and enclose the spongey urethra. 02:19 So what’s going to happen thereafter is that we have glands developing off the endoderm of the urogenital sinus. 02:27 So any gland associated with the bladder or the urethra actually has an endodermal origin from the urogenital sinus. 02:35 Now, moving forward, we’re now going to see how the bladder develops and enlarges. 02:43 Now, as the body gets larger, it needs to accommodate a greater volume of urine coming from the kidneys. 02:49 Initially, the urogenital sinus can handle whatever volume is coming in but it’s going to need to enlarge, and rather than just ballooning, it enlarges by pulling a portion of the mesonephric duct into its wall. 03:02 Now, if you have viewed the talk I did on development of the kidneys, you’ll know that the ureteric bud comes off the mesonephric duct and as the bladder enlarges, it pulls the mesonephric duct and the ureteric bud into its own wall and the smooth nature of those ducts is what makes the smooth trigone of the bladder on its posterior side. 03:25 So that’s what leads to the ureters emptying directly into the bladder. 03:31 In women, the mesonephric ducts go away. 03:34 In men, they are maintained as the vas deferens, also known as the ductus deferens. 03:39 And if we have a ductus deferens present entering the posterior side of the prostate and thereafter, the urethra, it’s going to drape over the ureter prior to doing so. 03:50 And if you have to locate and isolate the ureter from the vas deferens, you want to note that the vas deferens is going to drape over it on its way out to the testis. 03:59 Malformations involving the urogenital sinus largely cluster around failure of the allantois to rescind properly. 04:07 If the allaintois does not form a fibrous urachus leading to the top of the bladder, we can have a variety of problems. 04:14 Most prominently is a urachal fistula in which there’s an inappropriate connection between the urinary bladder and the umbilicus and in an infant who is born with urachal fistula, you will have urine dribbling out of the umbilicus. 04:30 Not quite as severe can be deep pouches leading from the umbilicus into the body or from the bladder up along the edge of your body wall. 04:40 Those are going to be umbilical urachal sinuses. 04:43 If it’s going from the umbilicus, in, or if it’s going from the top of the bladder out, that is gonna be called a vesicouracheal diverticulum. 04:52 Now, neither of these are particularly problematic because you don’t have urine drain into the umbilicus and may be relatively hard to catch because they don’t cause too many problems. 05:02 However, you can also have cysts develop where the allantois did not fully rescind and become urachus and those fluid filled cysts can be relatively non-problematic unless they get inflamed, and enlarged, and cause pain. 05:18 Other problems in this area involve the failure of the ureteric buds to enter the posterior side of the urinary bladder appropriately. 05:27 This is most common when we have an ectopic ureter form from a double ureteric bud. 05:33 Now, an ectopic ureter is a ureter that is emptying urine into the wrong location. 05:39 Most commonly, with these double ureteric buds will have one enter the bladder appropriately and the other will enter another nearby area inappropriately. 05:50 In particular, it may enter the urethra and since the bladder is there to store urine and only release it when the muscles that are at its base relax and allow urine to flow, there’s going to be a constant dribble of urine from the urethra into the vestibule or out the shaft of the penis. 06:10 In this case, it may actually be relatively hard to spot if an infant has this because you don’t typically notice if urine is constantly dribbling from an area. 06:19 You just notice whether the child has wet diapers or not. 06:22 But if a child has consistently always got wet diapers even a few weeks into development, it may be something to keep on your radar that there could be a problem with an ectopic ureter releasing urine constantly. 06:35 In women, the same process can occur but the ectopic ureter instead of releasing into the urethra can release into the vagina. 06:43 The net effect clinically will be about the same. 06:46 A constant dribble of urine but instead of from the urethra, it will be coming from the vagina and it is also possible to have ectopic ureters release onto the rectum. 06:56 Although, that is far less common because of the proximity difficulty there. 07:01 It’s hard for the ureter to make it all the way back to the rectum. 07:05 Thank you very much for your attention and I’ll see you on our next talk.
About the Lecture
The lecture Partitioning and Malformations of the Urogenital Sinus by Peter Ward, PhD is from the course Development of the Abdominopelvic Region. It contains the following chapters:
- Development of the Microscopic Kidney
- Malformations of the Allantois and Urachus
Included Quiz Questions
Which of the following best describes the allantois?
- A thin layer of endoderm that remains attached to the apex of the urogenital sinus and extends into the umbilical cord
- A common chamber that drains the GI and urogenital systems
- A mass of mesenchymal tissue that moves down to form a region of connective tissue at the perineum
- A region of mesenchymal tissue separating the rectum and urogenital sinus
- A structure that will ultimately become the prostate gland in men and the urachus in women
Any gland associated with the bladder or urethra has an origin of which cell type from the urogenital sinus?
- Endodermal
- Mesodermal
- Ectodermal
- Neural crest
- Mesonephric
During development what is the fate of the mesonephric ducts?
- In men, they become the vas deferens and in women, they recede.
- In men and women, they become the vas deferens.
- They become collecting ducts.
- They recede in both men and women.
- They become the ureters.
If the allantois does not disappear in a normal developmental manner, a variety of problems can occur; which of the following is not one of those problems?
- Ectopic ureter
- A blind pouch extending from the umbilicus or apex of the bladder
- A vesico-urachal diverticulum
- Urachal cysts
- An umbilical urachal sinus
Author of lecture Partitioning and Malformations of the Urogenital Sinus

Peter Ward, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
