Playlist
Show Playlist
Hide Playlist
Neurofibromatosis Type 1: Diagnosing Criteria

-
Strowd CNS Tumors Inherited Tumor Syndromes.pdf
-
Download Lecture Overview
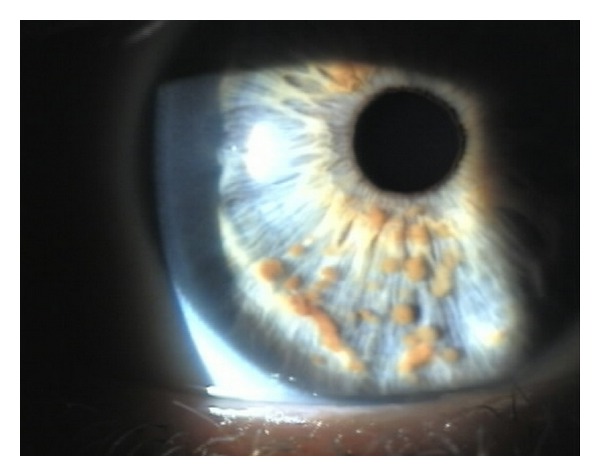
00:01 These are all genetic conditions and we're going to learn about the genetics of NF1 and NF2. 00:06 First, we'll focus on NF1. 00:08 NF1 results from a mutation in the NF1 gene. 00:12 The NF1 gene encodes a protein called neurofibromin, which you see here. 00:16 And neurofibromin is a break. 00:18 It is a tumor suppressor, it slows down growth. 00:21 And when it's normally functioning in the cell, the RAS pathway, which is the most common cell proliferation pathway is slowed down. 00:29 RAS cannot cause the cells to grow. 00:32 When you lose neurofibromin, cell growth is uninhibited and cells are able to grow. 00:38 And one of those cell growth signals is MEK. 00:40 And we're going to come back to this at the end of the lecture when we talk about treatment. 00:44 But that's an important downstream protein that causes cells to grow and proliferate and contributes to tumor formation in neurofibromatosis type 1. 00:55 So how do we diagnose patients within NF1? Well, it's a genetic condition, but we actually often don't test the genes. 01:02 We can... 01:03 we can look for that specific mutation in the NF1 gene that's causing this condition. 01:07 But as I said, it's one of the most, it's one of the biggest genes in the human body. 01:12 And it's very difficult to test all of the mutations that may occur. 01:16 So primarily, we rely on a clinical diagnosis. 01:19 And there are seven features that I want you to think about when making a clinical diagnosis of NF1. 01:25 The first are Cafe-au-lait macules. 01:27 And we saw those in an image and we'll look at a few more. 01:30 And six or more cafe-au-lait macules is sufficient to make a diagnosis or part of a diagnosis of NF1. 01:36 In prepubertal individuals, those must be greater than five millimeters and postpubertal individuals greater than 15 millimeters. 01:44 The second criterion are neurofibromas. 01:47 And we also looked at those for our patient. 01:49 Those are the lesions that we see out on the skin, the bumps. 01:52 And two or more dermal neurofibromas or one plexiform neurofibroma is sufficient for a major criteria for diagnosing neurofibromatosis. 02:01 We'll look at axillary and inguinal freckling or skinfold freckling, which is also one of the seven criteria. 02:07 Optic pathway gliomas. 02:09 Lisch nodules, which was present in our patient in case. 02:12 Osseous abnormalities. 02:14 We'll talk about sphenoid winged dysplasia, and pseudarthrosis. 02:18 And a family history. 02:20 Patients must have two of these seven criteria to be clinically diagnosed with NF1. 02:27 There are also additional symptoms and signs that we can see in these patients. 02:30 That aren't sufficient to establish a diagnosis, but can be highly contributing to the evaluation and management of these patients. 02:39 Cardiovascular malformations can occur. 02:40 We think of coarctation of the aorta or renal artery stenosis, which can occur later in life or in adolescent individuals. 02:47 Learning disabilities are extremely common in these patients and occur in up to 75% of this group of patients. 02:54 ADHD, Attention Deficit Disorder, as well as Hyperactivity Activity Disorder is also common. 03:00 Osteoporosis in Peenya, thinning of the bones, pectus excavatum, which is invagination of the sternum. 03:07 Bony abnormality that can occur. 03:09 Pheochromocytoma is another tumor that occurs on the adrenal glands and can cause elevated high blood pressure in these patients. 03:16 Glomus tumors on the skin or under the nails. 03:19 Gastrointestinal stromal tumors those are called GIST tumors, neat tumors that occur in the GI tract and are uncommon but can be seen in NF1. 03:28 Juvenile myelomonocytic leukemia, which is a very difficult to complication of this condition. 03:33 It's rare, but can occur in young adolescents. 03:36 Dural ectasia, scoliosis, and early onset breast cancer. 03:40 So almost all organ system can be involved in NF1. 03:44 And we're going to focus on those that establish the diagnosis and other principal organs to be affected.
About the Lecture
The lecture Neurofibromatosis Type 1: Diagnosing Criteria by Roy Strowd, MD is from the course CNS Tumors.
Included Quiz Questions
Which of the following is one of the seven criteria for the diagnosis of neurofibromatosis type 1?
- Osseous lesion
- Bilateral acoustic schwannoma
- A unilateral port-wine stain
- Facial angiofibroma
- Hypomelanotic macule
Which of the following tumors is most associated with neurofibromatosis type 1?
- Pheochromocytoma
- Wilms tumor
- Rhabdomyoma
- Liposarcoma
- Medullary thyroid carcinoma
Which of the following dermatological findings is most associated with neurofibromatosis type 1?
- Axillary freckling
- Alopecia
- Cavernous hemangioma
- Acne vulgaris
- Shagreen patches
Author of lecture Neurofibromatosis Type 1: Diagnosing Criteria

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
I like that NF-1 and NF-2 are compared on the same slide.
