Playlist
Show Playlist
Hide Playlist
Myocarditis: Signs, Diagnosis & Management


-
Slides Myocarditis InfectiousDiseases.pdf
-
Reference List Infectious Diseases.pdf
-
Download Lecture Overview
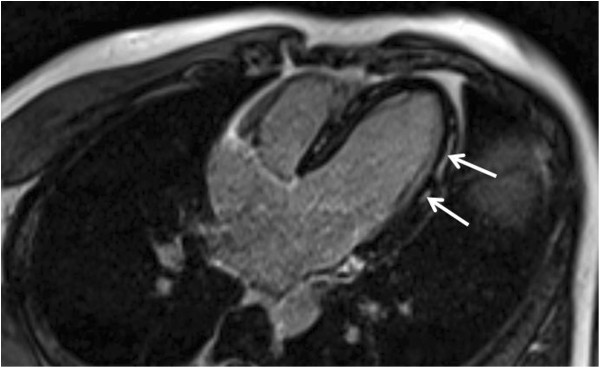
00:00 The clinical features of myocarditis are widely ranging. You can have, for example a completely asymptomatic patient who’s got really a subacute infection to someone who’s got a rapidly fatal fulminant myocarditis with heart failure. When should your clinical suspicion be aroused, unexplained heart failure, for example in a young person, someone with no predisposing problems like hypertension, myocardial infarction. 00:41 Also, you should suspect it in somebody who’s got chest pain. It can actually mimic the pain of acute myocardial infarction. Someone who comes in with a supraventricular tachycardia, they’ve never had problems with arrhythmias before. Now, they’ve got a rapid heart rate with multiple ventricular extrasystoles. That just doesn’t happen in normal individuals; or cardiac abnormalities developing during a recognized systemic infection. So a patient comes in, for example, the typical viral syndrome and then they proceed to heart failure, arthralgias, respiratory symptoms along with it. 01:30 So, how do you make the diagnosis? Well, it’s usually a diagnosis that’s presumptive based on the patient’s age, exposure history, and the clinical course. The workup would include a CBC. 01:47 It would be rheumatologic screening to rule out connective tissue diseases. Certainly, you want to get cardiac enzymes including troponin I. An echocardiogram is definitely indicated to look for other causes, valvular, congenital, amyloid heart disease. When available, you would want to get serum viral antibody Obviously, you want to follow and monitor the electrocardiogram. When available, you would want to get serum viral antibody titers, acute and convalescent. There is available non-invasive cardiac imaging. For example, cardiac MRI can reveal changes within the myocardium itself consistent with viral myocarditis. We are now doing more and more endomyocardial biopsies with viral genome testing. But the problem with that is you do that through a catheter and there’s sampling error that may be involved. 02:52 How do you manage myocarditis? It’s essentially supportive therapy in hemodynamically stable patients. The patients who have heart failure have to be given ACE inhibitors, β-adrenergic blockers. 03:09 Anti-viral therapy, much as we’d like to have it has very limited applications in myocarditis. 03:16 I’m not aware of any studies showing efficacy in a major way of any anti-viral drug. 03:24 For Trypanosoma cruzi, Chagas disease, the treatment of choice is benznidazole or alternatively nifurtimox. You may get substantial resolution of this problem with these agents. 03:41 Immunosuppression has been tried but it certainly could not be considered useful routinely. 03:48 There are too many problems with immunosuppression especially with agents like corticosteroids which may cause retention of fluid, aggravate heart failure. With things like methotrexate and other chemotherapeutic agents that suppress the immune system, we are just not, they’re not ready for prime time, not ready for routine use. That concludes my discussion of myocarditis. 04:15 I hope it was somewhat helpful to you.
About the Lecture
The lecture Myocarditis: Signs, Diagnosis & Management by John Fisher, MD is from the course Cardiovascular Infections. It contains the following chapters:
- Myocarditis – Signs/Symptoms
- Myocarditis – Diagnosis
- Myocarditis – Management
Included Quiz Questions
Which of the following patients most likely has viral myocarditis?
- A young patient with unexplained heart failure
- An elderly woman with heart failure and a history of myocardial infarction
- A patient with chest pain when lying down or taking deep breaths
- An elderly patient with new atrial fibrillation
- A 48-year-old man with ventricular tachycardia and diabetes
Which of the following medications is most appropriate in a patient with heart failure due to myocarditis?
- Angiotensin-converting enzyme inhibitors
- Antiretrovirals
- Nonsteroidal anti-inflammatory drugs
- Alcohol
- Exercise
Which of the following is the most appropriate recommendation for most patients with the indeterminate form of chronic Trypanosoma cruzi infection?
- Benznidazole
- Supportive care
- Anithypertensive medication
- Non-steroidal anti-inflammatory drugs
- Corticosteroids
Author of lecture Myocarditis: Signs, Diagnosis & Management

John Fisher, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
