Playlist
Show Playlist
Hide Playlist
Myocarditis: Definition and Epidemiology


-
Slides Myocarditis InfectiousDiseases.pdf
-
Reference List Infectious Diseases.pdf
-
Download Lecture Overview
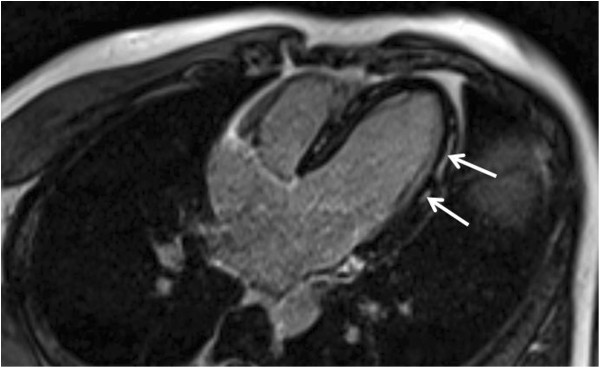
00:01 Continuing our discussion of cardiovascular infections, we turn now to myocarditis. 00:08 And myocarditis is a clinical syndrome due to myocardial injury and inflammation. 00:14 And it can be caused by a wide variety of infectious microorganisms. 00:22 And I'm showing you sort of the end stage of a dilated cardiomyopathy. 00:30 And this is caused in about 10% of the cases by viruses. 00:35 So this is what you would expect in patients who don't recover from viral myocarditis. 00:45 The incidence of myocarditis is uncertain, but the disease certainly is rare. 00:52 And it's very difficult to make a specific microbiological diagnosis for the same reason that viruses. 01:01 Many viruses can do this. 01:04 And figuring out which virus did it is very, very difficult. 01:09 Viral cultures are not often done. 01:12 It's just a difficult problem. 01:14 Males are affected more than females, and it actually is the most common cause of unexpected exercise related death in the US Air Force recruits. 01:26 So that's still going to be rare. 01:29 Unexpected death on a recruit is rare, but that's where viral myocarditis explains many of the cases. 01:40 So if you take home the message that viruses most commonly do this and there's an entire laundry list of them, there's enteroviruses, adenovirus, parvovirus B 19, human herpesvirus 6, dengue viruses, cytomegalovirus, coxsackievirus, which is notorious poliovirus, and even HIV, has been associated with myocarditis. 02:10 Unfortunately, there's not very much that we can do about viral myocarditis, except to support the patient. 02:20 Bacterial infections are only occasionally associated with myocarditis and usually result from either bacteremia, direct extension from a contiguous focus, say in the lung or mediastinum somewhere, or from the effects of a bacterial toxin. 02:41 The leading parasite to cause this problem is Trypanosoma cruzi, which causes what we call Chagas disease. 02:51 And there are a variety of miscellaneous noninfectious causes, such as chemotherapy for cancer or variety of drugs. 03:02 Ethanol, unfortunately, is is still a pretty common cause of dilated cardiomyopathy. 03:10 Allergic reactions post transplant rejection explains a fair amount of this problem. 03:16 And cardiac transplants and autoimmune diseases. 03:22 During the pandemic era, medical surveillance detected increased myocarditis cases in young people aged 12 to 30, with some data suggesting a link to mRNA vaccines. 03:32 Like many emerging medical observations, this remains an active area of study as scientists work to fully understand the relationship. 03:41 In discussing the pathogenesis, I'm showing you essentially two panels on the left. 03:47 You see the effects of viral myocarditis. 03:52 And I think you can see the myocardial cells are infiltrated with innumerable round cells, both lymphocytes of the T cell variety and B cell variety. 04:09 And it is these cells which injure the cardiac myocytes. 04:16 On the right panel, you're looking at the infiltration of the parasite into the myocardial fibers. 04:26 These are the amastigotes of Trypanosoma cruzi causing a similar process as viral myocarditis. 04:39 First of all, the pathogenesis would involve invasion of the myocardium from the bloodstream by the virus or by a toxin, and direct myocytes death from viral damage itself from cytolytic T cells or from apoptosis. 05:03 As part of the immune system process, you end up with decreased regulatory T cell function, activation of cytolytic T cells, and an increased influx of Th1 and Th2 cytokines. 05:22 The cytokines actually further damage the cells. 05:27 Moreover, the antigen presenting cells stimulate a pathogenic response from T cells and antibodies to the pathogens may cross react with endogenous epitopes, and you get epitope spreading between endogenous myocardial epitopes. 05:48 And so you can either resolve the infection and clear the virus and down regulate the immune response. 05:56 Or alternatively, you have ongoing injury because you have persistent viral infection or you've got a damaging immune response. 06:05 So it's hard to distinguish whether the virus is still active or whether it's the immune system that's further damaging the cardiac myocytes.
About the Lecture
The lecture Myocarditis: Definition and Epidemiology by John Fisher, MD is from the course Cardiovascular Infections. It contains the following chapters:
- Myocarditis – Definition and Epidemiology
- Myocarditis – Etiology
- Myocarditis – Pathology
Included Quiz Questions
Which of the following statements is most accurate regarding the pathogenesis of myocarditis?
- Damage to myocytes can result from the pathogen and/or the immunologic response to the pathogen.
- Damage to myocytes only results from the pathogen.
- Damage to myocytes only results from the immunologic response to the pathogen.
- Damage to myocytes is idiopathic and does not result from the pathogen or the immunologic response to the pathogen.
- The myocytes are not damaged during the pathogenesis of myocarditis.
What is the cause of Chagas disease?
- Trypanosoma cruzi
- Polio virus
- Dengue virus
- Entamoeba histolytica
- Giardia lamblia
Author of lecture Myocarditis: Definition and Epidemiology

John Fisher, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
