Playlist
Show Playlist
Hide Playlist
Mitral Stenosis and Mitral Regurgitation – Valvular Heart Disease

-
Slides Valvular Heart Diseases.pdf
-
Reference List Cardiology.pdf
-
Download Lecture Overview
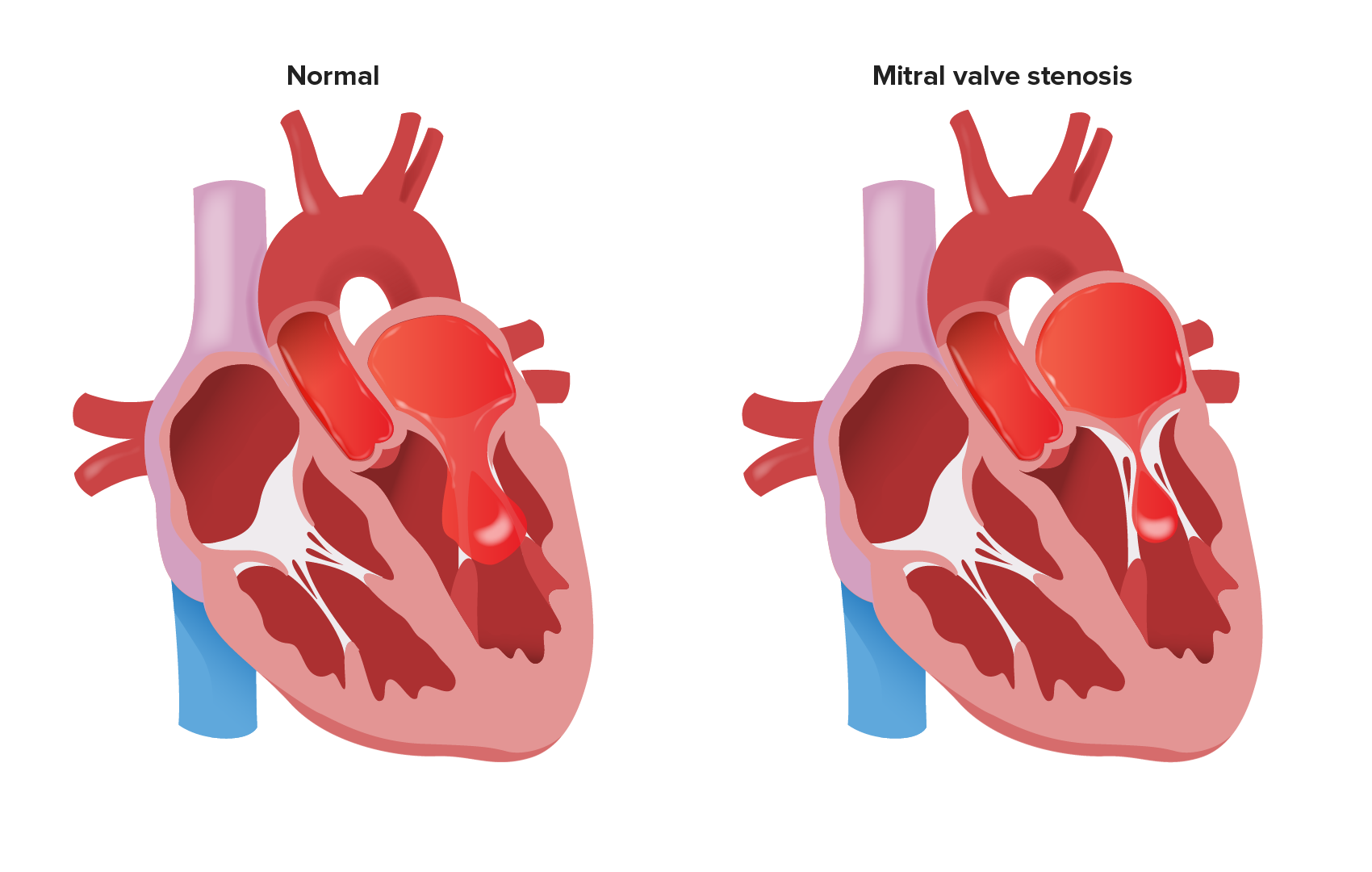
00:01 Alright, now let’s talk for a few moments about mitral stenosis. This used to be the commonest form of valvular heart disease when I was in training many years ago. But, because of the decrease in acute rheumatic fever, we don’t see mitral stenosis very much anymore. Why does the valve get stenotic in a patient who has acute rheumatic fever as a child? It’s an unfortunate event. When the body builds antibodies against the streptococcal germ which is the cause in many children of a strep throat, of a severe strep… infection in the throat, the antibodies that are developed actually cross react with the surface elements in the aortic and the mitral valves. 00:45 Consequently, there is a small amount of injury to the mitral and aortic valves during the bout of acute rheumatic fever. And this small injury builds up over the years as the valve continues to open and close, open and close. So, eventually, you end up with a highly scarred valve like you see here. The mitral valve normally has two nice thin leaflets and here you can barely make out which leaflet is which because of the severe thickening and calcification that has resulted from many, many years of use of the valve after its initial injury during acute rheumatic fever. 01:26 These days, actually, before you have to replace the valve, we can often open it if it isn’t too scarred with a balloon procedure, that is a catheter is snaked across the mitral valve with a deflated balloon. The balloon is inflated and it cracks the valve open. 01:42 And you can see the results here from one series, three years after the procedure, the gradient that is a… which is a measure of obstruction has not increased very much and actually, the valve area hasn’t changed much. And actually, after the balloon procedure, most patients do well for somewhere between five, seven, eight years. 02:03 And in fact, the nice thing about the balloon is you can do it again. Usually, the patients don’t do quite so well, but they gain another three or four years. Now, with two balloon procedures, you’ve pushed the patients out 10, 12 years before they need a valve replacement, which is a good thing. That’s all I’m going to say about mitral stenosis. We don’t see it a lot, when I see it in my home state of Arizona, it’s almost always in an individual who’s lived south of the border, in Mexico, Central America or Latin America and where they didn’t have good pediatric care that is they didn’t get penicillin when they developed a streptococcal sore throat and so, they did have acute rheumatic fever. As I said before, North America, Western Europe, it’s much, much, much less common. 02:47 There’s just an occasional case of rheumatic fever and these patients are treated very quickly and usually, put on penicillin for a long time to prevent recurrences with the end result that they do very well. Well, let’s talk about mitral regurgitation. 03:02 We talked about aortic stenosis and aortic regurgitation, talked about mitral stenosis, now we’ll talk about mitral regurgitation. The commonest causes of mitral regurgitation are congenital and coronary artery disease. Here in this picture, we see a patient… from... an autopsy picture of a patient with congenital myxomatous degeneration. That is in which there’s a lot of extraneous material that gets into the mitral valve. It’s a congenital inherited condition and you can see that the valve might function very abnormally because it’s all thickened and filled with this mucinous, mucus like material which renders the valve abnormal. The valve leaks and as I’m going to show you, most patients with this do pretty well. They're at increased risk for germ infections - for endocarditis, but in fact, relatively few need to go on to valve replacement. In this patient, valve replacement should have been done because you can see the little cords that hold the valve to the myocardium, one of them has ruptured resulting in acute mitral regurgitation. Acute mitral regurgitation is just like acute aortic regurgitation. It is poorly tolerated whereas chronic mitral regurgitation, the heart is able to compensate and many of these patients can go for decades without needing a replacement or a repair of the mitral valve. In these patients… some of these patients with myxomatous degeneration, the valve can be repaired and doesn’t have to be replaced. 04:37 Here is an echocardiogram showing you the valve prolapsing, that is the myxomatous valve falling back into the left atrium. You can see the little arrow. The valve should be straight across there not falling back into the left atrium, labeled LA from the left ventricle during ventricular systole. Now, it turns out that when one of these little cords that holds the mitral valve to the ventricular muscle breaks and the patient develops acute mitral regurgitation, medical therapy does not work. Again, no surprise, the acute load on the ventricle really requires a valve either repair or replacement and you can see here in a series from the Mayo Clinic, patients who underwent surgery did far better in the longer term follow up than patients who did not undergo surgery and only had medical therapy. 05:32 So, this brings us to the end of mitral regurgitation. Couple of points ought to be made again. 05:37 First of all, when a patient, for example, with myxomatous valve disease has a ruptured cord, the acute mitral regurgitation is poorly tolerated compared to the very well tolerated chronic mitral regurgitation. Secondly, mitral valve repair is possible in patients with myxomatous degeneration and younger patients do better with mitral valve repair than with mitral valve replacement. Rheumatic heart disease, mitral regurgitation usually is not amenable to surgical repair because the valve is too damaged. 06:11 In elderly patients, when you replace the mitral valve either for repair… with repair or replace the valve, it doesn’t make much difference in terms of the outcome. It’s just in younger patients that repair works better than valve replacement. 06:30 So, let’s go on now and speak about what chance the patient with myxomatous degeneration actually need surgery. Here’s a series from Australia where a large number of patients were followed in a special mitral valve prolapse or mitral valve myxomatous degeneration clinic and you can see, it’s only a few percent. But interestingly enough, a little more common in men than women and the replacement indication was, of course, the development of heart failure or acute mitral regurgitation with a ruptured cord. But even so, you can see over many years, it was still a very small percentage that actually needed valve replacement. And again, just to point out the statistics, why patients with severe acute mitral regurgitation do better with surgery and do better with repair than with replacement, particularly when the individuals are in middle life as opposed to quite elderly. 07:30 The major indication for surgery and patients with mitral regurgitation is the symptoms of heart failure. And again, we talked about acute heart failure from a ruptured cord is a strong indication for urgent valve, either repair or replacement.
About the Lecture
The lecture Mitral Stenosis and Mitral Regurgitation – Valvular Heart Disease by Joseph Alpert, MD is from the course Cardiac Diseases.
Included Quiz Questions
Which of the following is the most common cause of mitral valve regurgitation in North America and Europe?
- Myxomatous degeneration
- Endocarditis
- Stenosis
- Calcification
- Rheumatic fever
What is the underlying pathophysiology of mitral valve damage in rheumatic fever?
- Cross-reactive antibodies targeting valve tissue
- Congenital mucinous infiltration of valve leaflets
- Bacterial colonization of abnormal valve tissue
- Antibody complexes depositing into tissues
- Reactivation of latent infectious organisms
What intervention provides the best outcomes in acute mitral regurgitation from chordae tendineae rupture caused by myxomatous degeneration?
- Valve repair/replacement
- IV nitroprusside
- Lisinopril
- Balloon dilation
- IV Furosemide
Author of lecture Mitral Stenosis and Mitral Regurgitation – Valvular Heart Disease

Joseph Alpert, MD
Customer reviews
2,3 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
2 |
This lesson was very poorly organized and somewhat confusing. The content was exposed in what appears to be an arbitrary order and no logical connection was present. We were burdened with the graphs of multiple epidemiological studies while other elements of the diseases such as clinical presentation and diagnosis were neglected. Nonsurgical therapy is mentioned on the slides but was not explained in the lesson
This lecture lacks depth and does not cover the conditions in depth (e.g. physical findings, acute vs chronic pictures, etc). It's under cardiology, so I do not understand why it feels like an introduction only.
I really like your classes Dr Joseph, they are really specific and useful
