Playlist
Show Playlist
Hide Playlist
Measles Virus – Paramyxoviruses

-
02-45 Paramyxoviruses.pdf
-
Download Lecture Overview
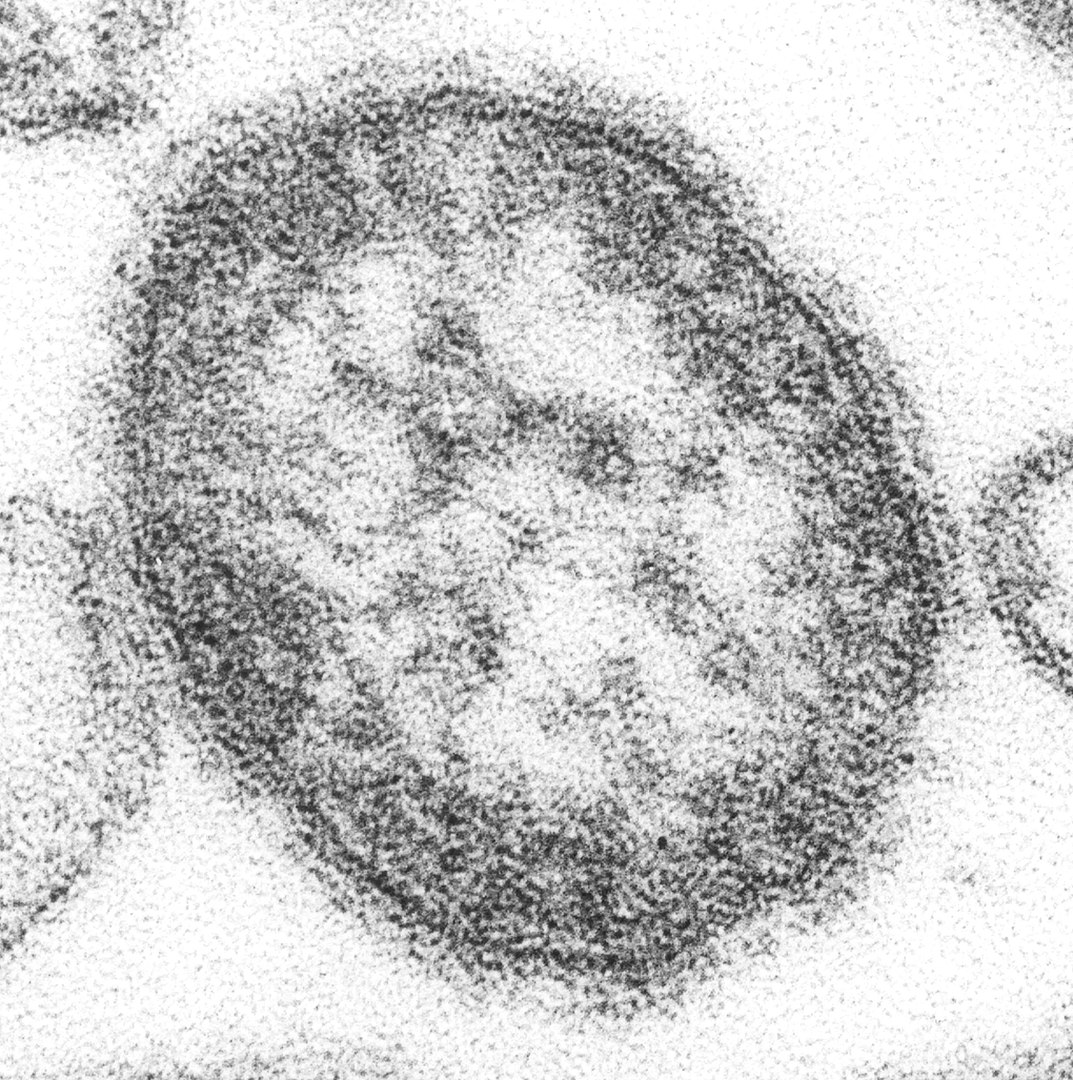
00:01 So, let's look first at measles virus. 00:03 This is a very, unfortunately, increasingly common virus in parts of the world where there are populations that are under vaccinated, currently, in the States and other parts of the world. 00:16 There's an incubation period of around 1-2 weeks, so 7-13 days, per the slide. 00:22 And after the initial infection of the upper respiratory tract and localized lymph nodes, with a secondary viremia, one can have attack to all the areas which you see in the slide. 00:33 So, the conjunctiva, the urinary tract, the small blood vessels, lymphatic system, even throughout the central nervous system. 00:41 And how far the viremia spreads and how aggressive it is, meaning that the viral load, really accounts for how severe the symptoms of the accompanying measles actually are. 00:53 So, what does measles look like? First, there is a prodromal period, which is very nonspecific. 01:00 However it -- I mean, it starts with fevers, malaise, etc., and then the patients develop the classic 3 C's: cough, coryza, conjunctivitis. 01:12 The cough. It's a brassy, deep cough, almost like a smoker's cough, which sometimes is productive of a deep sputum. 01:20 The coryza is typically starting as clear and then it becomes even a mucopurulent nasal discharge. 01:27 And the conjunctivitis. 01:29 Erythematous injection of the full conjunctiva with a very copious tearing of the eyes. 01:36 And along with that, sort of a photo phobia. 01:39 So, it's at this time that the patient may mistakenly be thought to have something like adenovirus, a cause of pink eye, or even influenza So it's still despite the presence of the classic 3 C's, a nonspecific presentation. 01:57 If one has a clinical suspicion, and if so, I take my hat off to you because it's hard to make that clinical judgment, but if one does, on day 3 of this prodromal period, one can start to see Koplik spots inside the mouth. 02:13 And with the picture in front of you, the dark arrow is showing one of those. 02:18 Koplik spots are sort of bluish-gray, small, like maybe 1 millimeter in diameter, papules on the buccal mucosa that have a slight surrounding red halo. 02:29 They're easy to miss unless you're specifically looking for them. 02:33 And if you see the Koplik spots in the setting of the 3 C's we just talked about, you have made your clinical diagnosis of measles. 02:41 Isolate and go on about your business. 02:44 However, many times, those presentations are missed, and then a maculopapular rash which has been nicknamed a morbilliform rash, a measles rash, kind of like defining it by the name of the infection, which is not very helpful. 02:59 But a densely erythematous, maculopapular rash starts and the distribution and progression is very key here. 03:08 It starts up at the head, starts cranially, and it moves caudally toward the tail, as it were, toward the extremities. 03:15 But there is a clearing of the rash as it moves from section to section over the period of 3-4 days. 03:23 So, with, still present, a conjunctivitis and one can see this dense, maculopapular rash on the face. 03:33 And then as it moves down toward the trunk, it may start to clear on the face and the conjunctivae may start to clear up as well. 03:40 By the time we get down to the lower abdomen and the pelvis, the areas of the neck and above may be either completely cleared or pretty close. 03:48 So, the progression is key to a clinical diagnosis of measles. 03:54 Unfortunately, there's no treatment. 03:56 There is prevention, as we'll talk about shortly. 03:59 But regardless of, you know, how severely ill or not severely ill the patient is, there are still complications. 04:08 These patients can progress to serious or severe measles, with pneumonia, These patients can progress to serious or severe measles, with pneumonia, with encephalitis, with seizures, with coma, the whole 9 yards. 04:18 And then after they've recovered from this spontaneously, and it may take several weeks for that, they are at risk for developing SSPE, subacute sclerosing panencephalitis. 04:30 This is a nasty. 04:31 This is very much, in appearance, like Alzheimer's disease, but it progresses, from start to finish, over a period of maybe months to at most, years, 1-2 years. 04:43 So think of these patients as losing cognition, losing awareness, losing body function, etc., but very, very rapidly. 04:52 So this is horrible. 04:53 And, of course, the whole thing is preventable via vaccine. 04:57 How to make the diagnosis. 04:59 Well, as mentioned, there -- I've given you multiple clinical clues. 05:02 The three C's: a progressive rash with clearing as one goes to the caudal region, and then, of course, the appearance of the rash itself. 05:12 But once one has a clinical suspicion, molecular diagnosis currently is the best way to go. 05:18 So an RT-PCR will pick up the RNA of the virus itself. 05:25 Transmission, as mentioned before, as with the other viruses, it's respiratory droplets. 05:30 Patients can be contagious prior to the onset of symptoms, prior to that prodrome, unfortunately, so during the incubation period of 1-2 weeks, patients can be infectious. 05:41 Which is unfortunate because it allows for epidemics or outbreaks of the disease to occur if one has a unvaccinated or under vaccinated population. 05:52 So, prevention, that vaccine. 05:55 Very effective. 05:56 A live, attenuated vaccine which we start to give to infants at 12-15 months of life with the booster at 4-5 years of life. 06:04 Currently, the vaccine is part of a combination vaccine, the MMR: measles, mumps, rubella, and all 3 are live and attenuated. 06:13 For patients who are unvaccinated, under vaccinated, maybe have only received 1 vaccine, or their vaccine status is unknown, if they are exposed to, in an epidemic setting, , a known case of measles, they can be given measles immunoglobulin. 06:31 So passive immunization to help them be protected, at least, for several weeks against developing further disease.
About the Lecture
The lecture Measles Virus – Paramyxoviruses by Sean Elliott, MD is from the course Viruses.
Included Quiz Questions
Which of the following refers to the approximate incubation period of measles virus?
- 7–13 days
- 1–4 days
- 14–18 days
- 19–24 days
- 25–30 days
Which of the following present as an early pathognomonic sign of measles appearing as bluish-gray grains of salt surrounded by a red halo on the buccal mucosa?
- Koplik's spots
- Roth spots
- Bitot's spots
- Forchheimer spots
- Canker sores
The typical type of rash observed due to infection by the measles virus is...?
- ...maculopapular.
- ...petechial.
- ...vesicular.
- ...eczematous.
- ...purpuric.
Which of the following is regarded as the most serious complication of infection by the measles virus?
- Subacute sclerosing panencephalitis
- Japanese encephalitis
- West Nile encephalitis
- Toxic-metabolic encephalopathy
- Wernicke encephalopathy
Author of lecture Measles Virus – Paramyxoviruses

Sean Elliott, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
