Playlist
Show Playlist
Hide Playlist
Intervertebral Disc and Neurologic Testing

-
Slides Osteopathic Diagnosis of the Lumbar Region.pdf
-
Reference List Osteopathic Manipulative Medicine.pdf
-
Download Lecture Overview
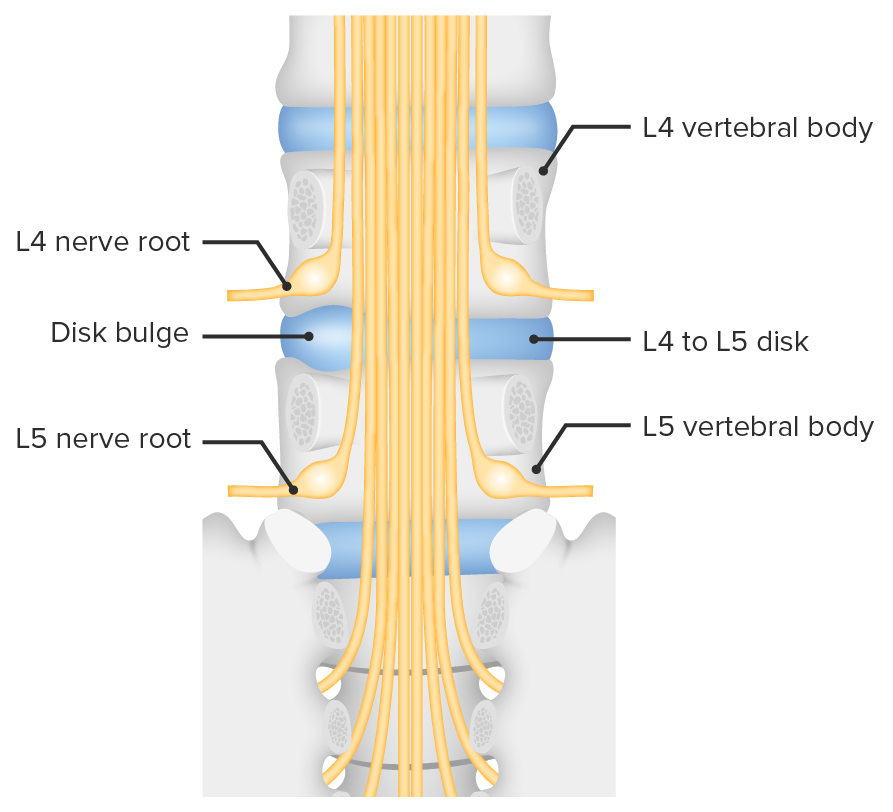
00:01 Low back pain is a very common presentation that physicians are encountered with. 00:06 When you have low back pain, on your differential is usually herniated disc. 00:11 So, in the lumbar spine, herniated disc is a very common occurence. 00:16 It's actually one of the more frequent occurences other than in the cervical spine at C5, C6. 00:23 So, our intervertebral disc consist of the annulus fibrosus and the nuclues pulposus. 00:28 The annulus is a fibrous ring and it's consist of interlocking crosshatch fibers. 00:35 And what happens is when you rotate right and left, those fibers will actually compress and get tighter. 00:42 It's also attached to the anterior and posterior longitudinal ligament. 00:46 The anterior ligament is really wide and broad and covers the anterior portion of the disc. 00:51 Whereas the posterior longitudinal ligament tends to be a little bit more narrow and thin. 00:55 This increases the risk of a posterior and lateral herniation which is the most common type of herniation. 01:01 The annulus fibrosus is also concave posteriorly. 01:06 Your nucleus pulposus is in the center. 01:09 This is made from the notochord. 01:10 It's surrounded by the annulus and it has reciprocal motion characteristics. 01:15 There's high water content there. 01:17 It's compressible and it relies on this pressure that you have when you move and compress and decompress throughout the day for nutrient and waste exchange. 01:29 So that reciprocal motion at the nucleus pulposus is that when I flex forward, that pulposus is actually driven posteriorly. 01:38 And when I extend, that nucleus pulposus is driven anteriorly. 01:41 So the most common cause of a herniated disc is flexing forward with your back and adding a stress or load to the spine. 01:50 So lifting something heavy and lifting up or actually lifting something heavy and twisting is really the worst motion and adds the most pressure to the back causing a potential herniated disc. 02:01 The lumbar spine has the nerve roots L1 to L5 passing through it. 02:07 This is important because it innervates most of the back and the lower extremities and the visceral organs, and a herniated disc could potentially compress on those nerves When you think of a disc herniation, it's important to know what level that disc herniation is occuring and what nerve is being compressed. 02:27 So when you're evaluating a patient, you're looking for key signs and symptoms and aspects of your physical exam which helps you to localize which nerve root is being compressed. 02:38 So if I have a disc herniation between two segments, it would usually herniate and entrap the nerve root of the segment below. 02:47 So in this case, in the image you could see how if I have a disc bulge between L4 and L5, it will compress the L5 nerve root because the L4 nerve root has already exited the spinal column away from the disc above it. 03:04 So, in order to assess if there is a neurologic deficit, there's many different types of testing that we could do. 03:10 The most common things that we check to make sure that the nerve root is intact or that the nerve is working well is to perform 3 main steps. 03:19 The first step is to check sensation. 03:21 So, these nerves innervate our skin and specific areas of the body will correlate with specific nerve roots. 03:29 So, in checking sensation, we could look to see if there's a loss of sensation to tell us if there's a compression or irritation that's compromising the nerve activity. 03:41 Reflexes could also be tested. 03:43 Certain reflexes will correlate with specific nerve roots. 03:47 The patellar reflex checking to see if your patella tendon reacts to a stretch is a testing for L4. 03:56 Your achilles reflex is testing S1. 04:00 Different nerve roots innervate muscles and so you could see associated muscle weakness when a certain nerve root is weakened. 04:08 A lot of our muscles actually have a mixed innervation, multi-levels. 04:12 So certain muscles could be a little bit more specific for key nerve roots but sometimes you may have a mixed pattern, so you may not see, necessarily note a lot of strength, lack of strength or weakness unless it's a very severe compression. 04:31 Straight leg raising is a test that you see in the image here. 04:35 Straight leg raising is a special test where we are applying a stretch on those nerves to see if that stretch will cause an irritation, so it is applied with the patient lying supine and you slowly bring the leg straight up in flexion to about 70 degrees. 04:55 If the patient could do that without pain, that's usually a negatve test. 04:58 If they're unable to tolerate that straight leg raise before they reach 70 degrees and they're having pain that shoots down the leg, not just tightness or pain behind the knee because of hamstring tightness, then that is a positive test. 05:14 So a positive test is shooting pain really going down the leg or like a numbness and tingling sensation. 05:20 If you are not sure if someone is malingering or pretending to have back pain due to secondary gain, what you could do is you could also perform this test with the patient seated. 05:31 So as they're seated, slowly straighten out their leg and this is actually going to give you the same amount of leg flexion as you extend the knee so the leg is straight. 05:42 And if they have the pain when they're lying supine, they should also have the pain when they're seated. 05:48 If they're malingering, then they might know the test to do the straight leg but not show the same reaction of pain when you straighten out their leg when they're in a seated position. 06:00 Here is the dermatomes. 06:02 As you could see, the dermatomes are overlapping at certain points. 06:07 So in order to be the most specific, you wanna test key areas especially for the lumbar spine. 06:13 So the lower lumbar segments tend to be the ones that are compressed the most often. 06:18 So typically, we're trying to differentiate between L4, L5 and S1. 06:25 So looking at the foot, if we are testing for L4, L5 and S1, you could look at the foot and check the medial foot for L4, the top of the foot for L5 and the lateral foot for S1.
About the Lecture
The lecture Intervertebral Disc and Neurologic Testing by Sheldon C. Yao, DO is from the course Osteopathic Diagnosis of the Lumbar Region. It contains the following chapters:
- Intervertabral Disc
- Lumbar Spine – Neurologic Testing
Included Quiz Questions
Which of the following is the most common direction of a spinal disc herniation?
- Posterolateral
- Anterolateral
- Inferolateral
- Superolateral
- Anterior
Which of the following nerve roots is being assessed when checking for the Achilles’ tendon reflex?
- S1
- S2
- L3
- L4
- L5
Which of the following nerve roots supplies the sensation to the medial aspect of the foot?
- L4
- L3
- L5
- S2
- S1
Author of lecture Intervertebral Disc and Neurologic Testing

Sheldon C. Yao, DO
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
