Playlist
Show Playlist
Hide Playlist
Interstitial Lung Disease (ILD): Overview

-
Slides 06 ILD InterstitialLungDisease RespiratoryAdvanced.pdf
-
Download Lecture Overview
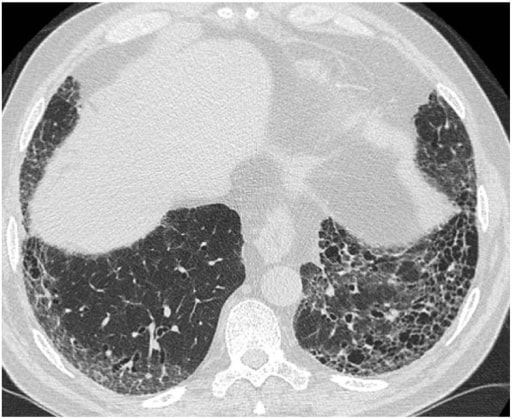
00:01 The subject of this lecture are interstitial lung diseases. These are non-infective, non-malignant infiltrations of the lung parenchyma. That is, they are diseases where the alveoli and the interstitium, the gap between the alveoli and the pulmonary capillaries and the rest of the lung is infiltrated by non-infective and non-malignant cellular content and extracellular components. There are a range of diseases which are in this category. The most important of which is lung fibrosis and sarcoidosis. In addition, there are diseases which are responses to inhaled substances and antigens such as hypersensitivity pneumonitis and pneumoconiosis, and a large range of unusual and very rare interstitial and infiltrative lung diseases which are normally included in the ILD category. 00:49 In general, ILDs, interstitial lung diseases, cause a restrictive lung function pattern. 00:55 That is they reduce the FEV1 and the FVC. As you can see on this diagram on the right hand side here that the ratio between the FEV1 and FVC is often increased and in fact, total lung capacity is reduced as well. In general, CT scans are also essential for an accurate assessment of these types of diseases. Pulmonary fibrosis is often a progressive disease and is actually very difficult to treat. 01:26 Categorizing ILDs is not straightforward. This is one way of doing of categorizing ILDs and is a useful way of thinking about them in general. So for example, here we have five categories. On the right hand side, you have pulmonary fibrosis. That has several different causes. It could be idiopathic, which is the commonest cause. It means that we don’t know what’s causing it. Or it can be associated with connective tissue disease such as rheumatoid arthritis or dermatomyositis. In addition, there are ranges of other situations where pulmonary fibrosis develops such as radiotherapy, drug-associated, by various drugs after adult respiratory distress syndrome. The other categories are hypersensitivity pneumonitis, and these are the commonest causes of that of farmer’s lung and Bird Fancier’s lungs, and these are immune reactions to inhaled antigens and is a form of allergy. Sarcoidosis, the cause of which is unknown is a disease in which you get infiltration of the lungs with granulomas and that can present an acute disease or a chronic disease and it can have lung involvement, pulmonary sarcoidosis, or involvement of other organs, extra-pulmonary sarcoidosis. Then there are pneumoconiosis which is a non-allergic response to inhaled substances such as coal dust, asbestosis, which causes an interstitial lung disease of various different patterns depending on what the substance is that you are inhaling. 02:54 The last category here are the very rare diseases which I am not going to discuss in any detail today, which often cause cold interstitial lung disease but have their own distinct patterns and types of infiltrations. Now, very important components of this diagram are the arrows showing that patients with severe hypersensitivity pneumonitis, severe sarcoidosis,severe pneumoconiosis, and some of the other rare interstitial lung diseases with aggressive severe diseases, end up with what looks like pulmonary fibrosis at the end. So for example, if you have end-stage sarcoidosis, it actually looks clinically and radiologically, very similar to end-stage pulmonary fibrosis. And as a consequence, sarcoid, hypersensitivity pneumonitis and various pneumoconiosis are thought of as causes of pulmonary fibrosis. 03:45 Another important point from this slide is that there are old names to some of these disease. 03:49 For example, idiopathic pulmonary fibrosis used to be called cryptogenic fibrosis alveolitis. 03:54 And hypersensitivity pneumonitis used to be called extrinsic allergic alveolitis. 03:58 These terms are interchangeable now.
About the Lecture
The lecture Interstitial Lung Disease (ILD): Overview by Jeremy Brown, PhD, MRCP(UK), MBBS is from the course Interstitial Lung Disease (ILD).
Included Quiz Questions
Which of the following statements regarding pulmonary function tests in patients with interstitial lung disease are TRUE?
- FEV1/FVC is raised in comparison to healthy individuals.
- FEV1 is raised in comparison to healthy individuals.
- FVC is raised in comparison to healthy individuals.
- Total lung capacity is increased in comparison to healthy individuals.
- Transfer factor is increased in comparison to healthy individuals.
What condition do long-standing interstitial lung diseases resemble after prolonged courses?
- Pulmonary fibrosis
- Pneumoconiosis
- Hypersensitivity pneumonitis
- Berylliosis
- Eosinophilic pneumonitis
Author of lecture Interstitial Lung Disease (ILD): Overview

Jeremy Brown, PhD, MRCP(UK), MBBS
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
The teacher has great pronunciation! And classification made clear by extensive table.
