Playlist
Show Playlist
Hide Playlist
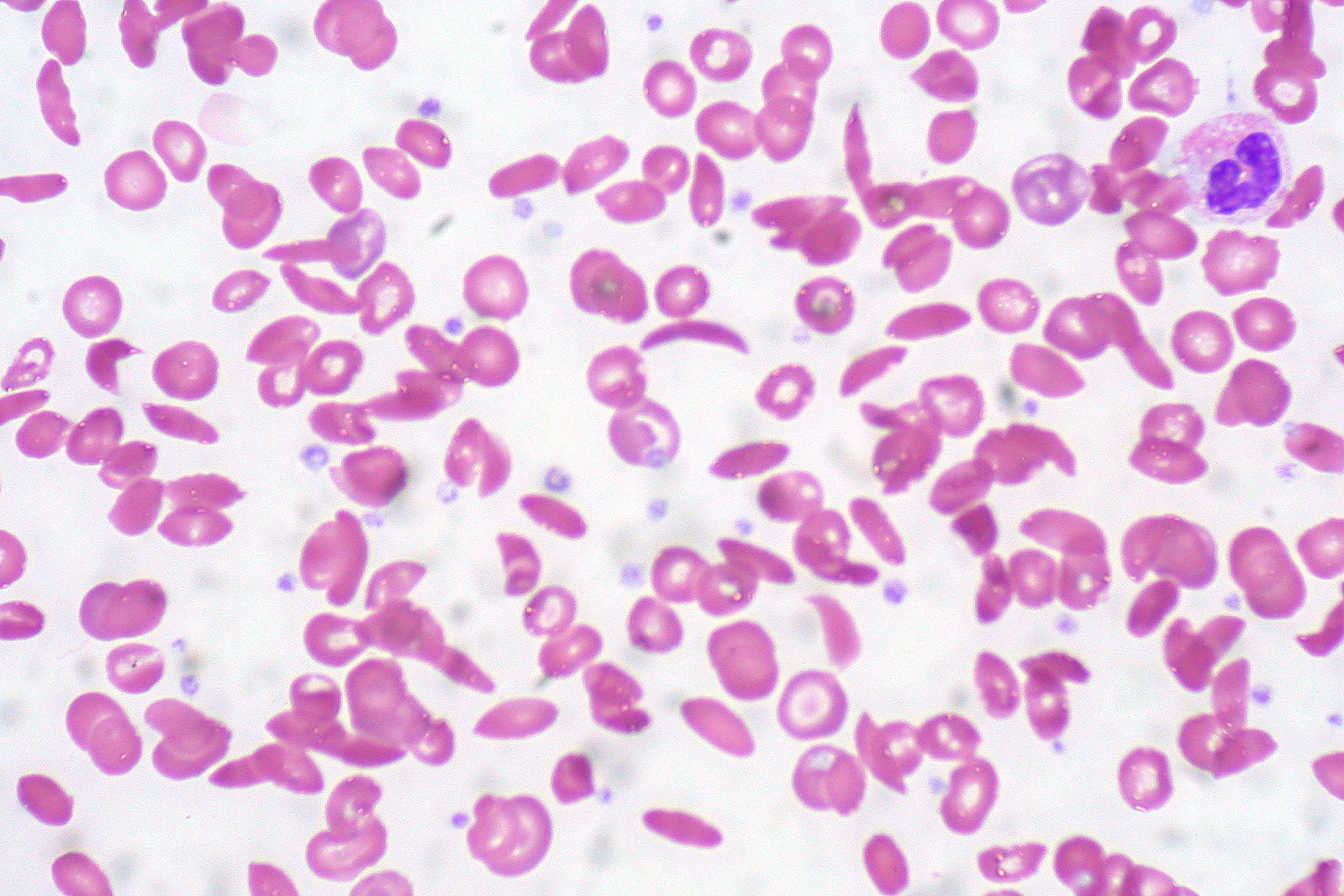
Hemoglobin SS Disease

-
Slides Sicklecelldisease Pediatrics.pdf
-
Download Lecture Overview
00:01 So how does hemoglobin SS disease, our classic presentation of sickle disease, how does it present? The most important thing that we should know about is the vaso-occlusive pain crisis. 00:13 This is common. 00:15 Patients with hemoglobin SS disease will present with extraordinary pain. 00:20 They often have to be treated with large amounts of morphine for comfort. 00:24 And this is a complicated problem because they may become addicted to morphine and it may be difficult to distinguish the pain crisis from non-pain crisis. 00:33 It’s important to know which patients have sickle cell disease though because pain is never a good option. 00:39 These patients also are at increased risk for stroke. 00:42 Remember, these sickled cells can cause microvascular trauma which can setup a hypercoagulable cascade. 00:50 So we need to be aware of these patients having sickle cell disease because they can have stroke even in childhood. 00:58 It’s common for patients to have an infarction of their spleen or splenic sequestration. 01:03 This usually happens very early in life from the first several years. 01:08 These patients may develop a large spleen, but then eventually that spleen will contract down and be essentially ineffective. 01:17 Acute chest is a significant problem. 01:20 This is when cells get sickled inside the lungs. 01:23 The problem is it can cause a fever and it can be clinically very challenging to distinguish acute chest from pneumonia. 01:30 So they often end up on antibiotics as well. 01:34 Patients may have myocardial dysfunction from clots, literally having a myocardial infarction. 01:41 Patients may develop priapism. 01:43 Any erection that lasts more than 4 hours must be attended to and generally, you have to do -- you have to call urologist who then can draw the blood out of the penis. 01:52 It’s very complex and challenging to deal with. 01:55 Patients may have an aplastic crisis. 01:58 In other words, they may have a moment when they stop making red blood cells inside their bone. 02:04 This may be a result of, say, a viral infection. 02:08 Additionally, patients can develop osteomyelitis or bone infections. 02:13 Normal patients can develop osteomyelitis too. 02:16 So the reason I bring this up is that because these patients are asplenic, they are at risk for unusually, a salmonella osteomyelitis. 02:25 In these patients, probably group A strep is still the most common organism, but when we see them with an osteomyelitis, we have to think of expanding our antimicrobial coverage beyond the usual culprits which are group A strep and Staph aureus. 02:40 Patients with hemoglobin SS disease eventually will develop chronic condition as well such as avascular necrosis of joint such as the hip. 02:49 They may develop cholecystitis from frequent red blood cell turnover resulting in gallstones and obstructive biliary tree disease. 02:57 Patients may develop hearing loss. 03:00 They may develop leg ulcers from inadequate perfusion of the extremities. 03:04 They develop retinopathy. 03:07 They also may develop renal failure from sludging within the kidneys. 03:11 They may develop liver cirrhosis and if the lungs continue to get acute chest syndrome, they may eventually develop a pulmonary hypertension.
About the Lecture
The lecture Hemoglobin SS Disease by Brian Alverson, MD is from the course Pediatric Hematology.
Included Quiz Questions
Which of the following is always an acute complication of hemoglobin SS disease?
- Priapism
- Avascular necrosis
- Leg ulcers
- Hearing loss
- Cirrhosis
Which of the following organisms is found more commonly in sickle cell osteomyelitis than in osteomyelitis in otherwise healthy patients?
- Salmonella
- Staphylococcus aureus
- Candida
- Group A streptococcus
- Escherichia coli
Author of lecture Hemoglobin SS Disease

Brian Alverson, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Excellent overview of the acute and chronic complications of the disease.
