Playlist
Show Playlist
Hide Playlist
Helicobacter Pylori Infection

-
Slides Stomach and Duodenum.pdf
-
Download Lecture Overview
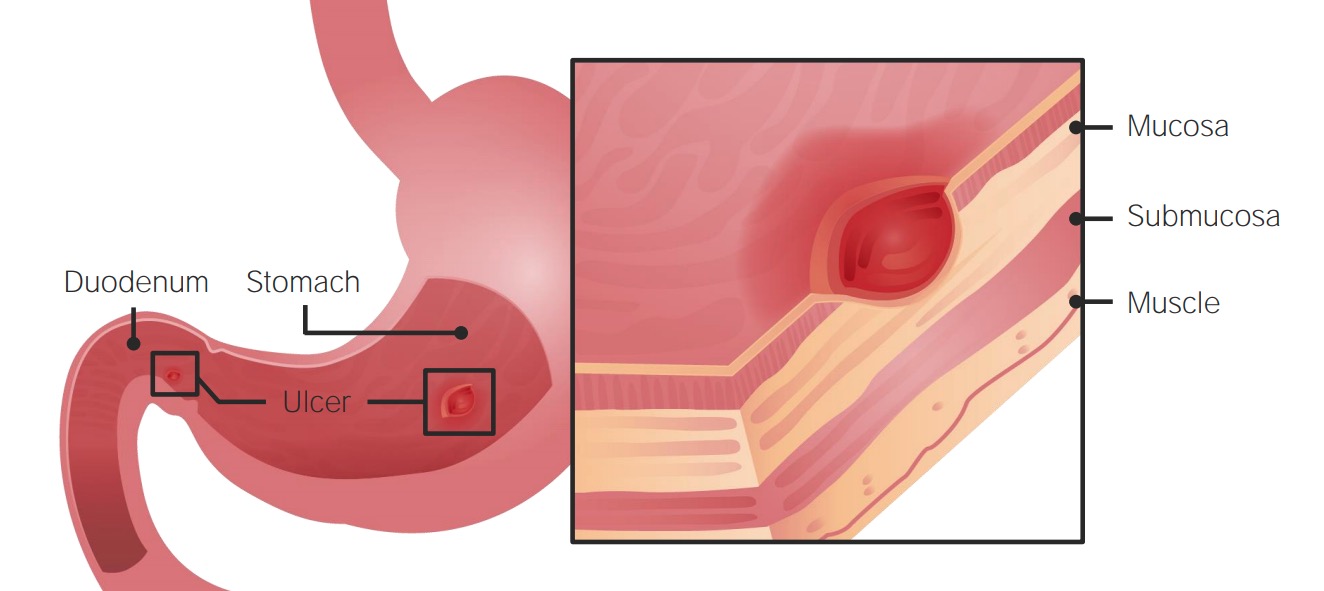
00:01 Let us now officially move in to H. pylori. 00:04 Remember that H. pylori is associated in both types of peptic ulcer disease. 00:08 It's a gram negative, comma shaped bacillus. Fecal-oral transmission. 00:14 Prevalence increases with age. 50% infection among the general population greater than 60. 00:21 Extremely common. High prevalence in developing countries, much more so. 00:26 Risk factors include low socio-economic status, increased population, institutionalization. 00:34 And by institutionalization, we mean that we're talking about a patient who might have had psychiatric issues therefore committed. 00:42 In those closed quarters, pretty sure that your patient will have H. pylori. 00:48 Look for such history in your patient. 00:51 Comma-shaped organism, flagellated. 00:55 It has urease activity so that it can then take the urea, produce the ammonia to protect itself. 01:03 Serology. IgG antibody always remains positive after eradication because this is long-term. IgG. 01:12 Urea breath test is important for diagnosis. High sensitivity and specificity. 01:18 Stop the PPI therapy because this then allows for the H. pylori to actually thrive. 01:27 Biopsy urease test. Instant result, low cost, but requires gastric tissue. 01:35 There is a stool antigen test useful for documentation of eradication. 01:40 Histology. Highest sensitivity and specificity. Tissue culture. 01:48 Cumbersome, used however for unfortunately, antibiotic resistance is part of reality. 01:55 Cumbersome but useful with refractory. 02:00 The combination antibiotic and anti-secretory agents result in eradication with the high percentage of your patient. 02:07 And it is that simple to be diligent about getting rid of your H. pylori so that you prevent perhaps cancers from taking place. 02:16 Metronidazole seems to be increasing with resistance. 02:19 Re-infection is always a possibility. 02:23 Not recommended for asymptomatic patients. 02:27 Now, briefly just management with antibiotics. 02:31 Bismuth, metronidazole, tetracycline, PPIs. 02:38 We have Lansoprazole plus Amox or amoxicillin, plus clarithromycin. 02:46 This is known as your PrevPac and the most widely used. 02:50 Please be familiar with one of these regimens or actually both of these regimens so that you eradicate your H. pylori effectively. 03:01 Associated disease with H. pylori. Both duodenal and gastric ulcers. 03:07 The type of what's known as your chronic atrophic gastritis, chronic atrophic gastritis. 03:18 A Helicobacter will give rise to Type B type of chronic atrophic gastritis. 03:27 The gastric primary adenocarcinoma that you're worried about specifically with H. pylori is called the intestinal type, not the diffuse. 03:37 So whenever you hear about signet-ring cells that are found in the ovaries, hematogenous metastasis of, that's a diffuse type of gastric adenocarcinoma. 03:49 With H. pylori, it will be the intestinal type and it will almost never move. 03:55 Another type of major, major GI cancer that H. pylori is associated with. 04:03 Hence, these two bullet points are huge for you and every form of medicine. 04:09 If you're able to properly get rid of the H. pylori, you might actually treat and prevent these two major cancers from developing. 04:19 The intestinal type of primary gastric adenocarcinoma number one. 04:23 And number two, we have a lymphoma called the mucosa associated lymphoid tissue-oma. 04:29 It's a lymphoma. Keep that separate from adenocarcinoma. 04:34 Two completely separate different types of cancers that H. pylori very much associated with.
About the Lecture
The lecture Helicobacter Pylori Infection by Carlo Raj, MD is from the course Stomach and Duodenum Diseases: Basic Principles with Carlo Raj.
Included Quiz Questions
What type of bacteria is H. pylori?
- Gram-negative
- Acid-fast
- Rod-shaped
- Cocci
What percentage of patients affected by H. pylori infections are older than 60 years of age?
- 50%
- 30%
- 40%
- 60%
- 70%
What is an effective test for detection of H. pylori infection?
- Urea breath
- Ultrasound scan
- Blood picture
- Urine analysis
- GFR
Author of lecture Helicobacter Pylori Infection

Carlo Raj, MD
Customer reviews
3,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
1 |
| 2 Stars |
|
0 |
| 1 Star |
|
1 |
too little information even about therapy and moa. Dr Raj is literally reading the slides. i can do it by myself.
good review of the topic. I am unsure why someone has given it 3 stars. Cant fault it.
It would would have been good to further elaborate on dx testing and in which clinical circumstances one would be more appropriate over the other. Also with the increasing incidence of resistant organisms I feel the lecture didn't adequately outline appropriate second line management. Also the error regarding PPI which was flagged by another listener
