Playlist
Show Playlist
Hide Playlist
Focal Segmental Glomerulosclerosis

-
Slides NephroticSyndrome RenalPathology.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
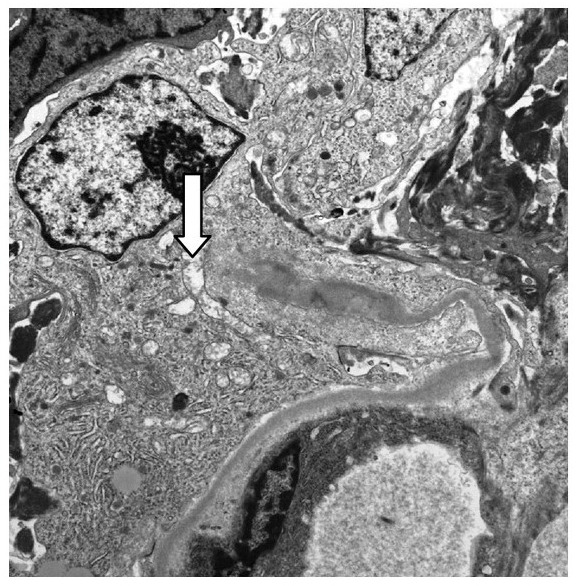
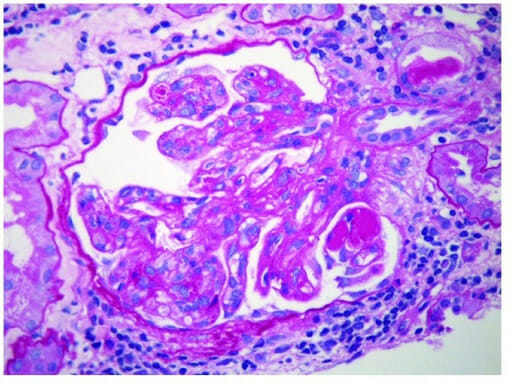
00:01 Let’s go on to our second type of nephrotic syndrome, this then brings us to focal segmental glomerulosclerosis. 00:08 Now, you’ll find this to be quite interesting and you must know this is quite important. 00:13 The reason I say that is the following. 00:15 There’s going to be primary secondary diseases of FSGS, Focal segmental. 00:21 And it’s important for us to point out when this occurs in your patient. 00:25 So let’s begin. At some point when we get into renal failure, we’ll take a look at the various stages of chronic renal failure. 00:36 And when we do so, we then have to walk through the different reasons and the different clinical scenarios and outcomes. 00:45 And when we do so, at some point in time, please understand that well, as we go through the classes that you might have enough damage but there's also a compensatory mechanisms. 00:57 When you start having compensating issues or effects of those glomeruli that are dying, the actual hypertrophy, you can call it, of the glomeruli, results in your focal segmented glomerulosclerosis. 01:13 And what that means is the following. 01:15 That few glomeruli are affected. Not all. 01:19 So is it possible that upon biopsy that you actually missed a diagnosis of FSGS? Sure, you can. 01:26 Next, well, when you take a look at that glomerulus, it’s not even the entire glomerulus that’s affected. 01:32 It’s only a segment of it. 01:34 That’s why we call it focal segmental glomerulosclerosis. 01:37 So many times, when you would find FSGS, is as, you have a patient getting older and has further disease process setting in, please understand that the remaining glomeruli may undergo compensation. 01:53 Interesting concept? You have to know it absolutely. 01:57 Is it relatively new to you? Well, that’s up to your medical education but please know it. 02:03 It’s extremely important. 02:04 Renal failure is a big part of our society. 02:07 Now, a secondary disease, HIV, the most common glomerular disease, in an HIV patient will be FSGS. 02:17 H, HIV. H, heroin abuse. 02:21 Wonderful habits for one to develop, isn't it? HIV and heroin resulting in secondary type of FSGS. 02:30 Here, once again, no immune-complex is therefore you’ll have a negative immunofluorescence. 02:37 But what do you find in electron microscopy? What’s VEC stand for? Visceral epithelial cells, aka, podocytes. 02:47 What is your primary sense or what’s your primary source of damage, is it cytokines or the neutrophils? Good. It’s cytokines. 02:55 Nonselective proteinuria, microscopic hematuria, could be present. 03:01 Hypertension, early. 03:03 Poor prognosis, commonly progresses to chronic renal failure. 03:08 As I said earlier, when you have the stages of end stage renal disease, please understand at some point the other glomeruli are going to undergo a step or stages of compensation. 03:20 Focal segmental glomerulosclerosis. 03:23 Corticosteroids, not as responsive as those patients receiving corticosteroids for minimal change disease. 03:29 That’s an important differentiation. Who is your patient? Older patient as he or she might be going into renal failure, end-stage renal disease then there would be other glomeruli that are doing what? Compensating, that is a very important pathogenesis. 03:44 Sclerosis of some glomeruli, focal, and only a portion involved. 03:50 What’s sclerosis mean? Thickening and narrowing. 03:54 So as I said earlier, is it possible that you might miss the diagnosis of your glomeruli because some might actually look normal? Yes, only a few might be involved. 04:07 And of the glomerulus that has been involved only a segment of it in fact is. 04:12 African-American have a genetic propensity to develop this syndrome. 04:17 Genetic, that’s unfortunate. Associations, secondary H. 04:21 HIV, one of the most common glomerulonephritis that an HIV patient would develop is FSGS. 04:27 Heroin, sickle-cell disease, and obesity could all be associated with FSGS. 04:34 What you're finding here is the following. 04:37 First and foremost you tell me, get on the pattern or organization of understanding what you're seeing. 04:43 This is light microscopy. H&E stain. 04:47 You tell me, does it look like the entire glomerulus has been affected? No. Only a segment of it is. 04:54 Is it possible in the same kidney in which you’ll then find a glomerulus which is normal? Sure. Remember some of the glomeruli may appear perfectly normal, so you wanna be really careful. 05:04 If you find your patient with a history of HIV, heroin, or even getting older with end-stage renal disease, keep in mind, that if you don’t find your first biopsy with their glomeruli being damaged, then you wanna make sure and see is to whether or not your diagnosis holds true as being clear for FSGS or in fact involving FSGS.
About the Lecture
The lecture Focal Segmental Glomerulosclerosis by Carlo Raj, MD is from the course Glomerulonephritis.
Included Quiz Questions
What is the most common glomerular disease in HIV?
- Focal segmental glomerulosclerosis
- Membranous glomerulonephritis
- Membranoproliferative glomerulonephritis
- Diffuse proliferative glomerulonephritis
- Minimal change disease
Which of the following is not seen in focal segmental glomerulonephritis?
- Selective proteinuria
- Hematuria
- Hypertension
- Chronic renal failure
- Nonselective proteinuria
Which of the following is not a likely association of focal segmental glomerulosclerosis?
- Hepatitis A
- HIV
- Obesity
- Sickle cell disease
- Heroin abuse
Author of lecture Focal Segmental Glomerulosclerosis

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
