Playlist
Show Playlist
Hide Playlist
Encephalitis: Examination

-
Slides CNS Infections Encephalitis.pdf
-
Download Lecture Overview
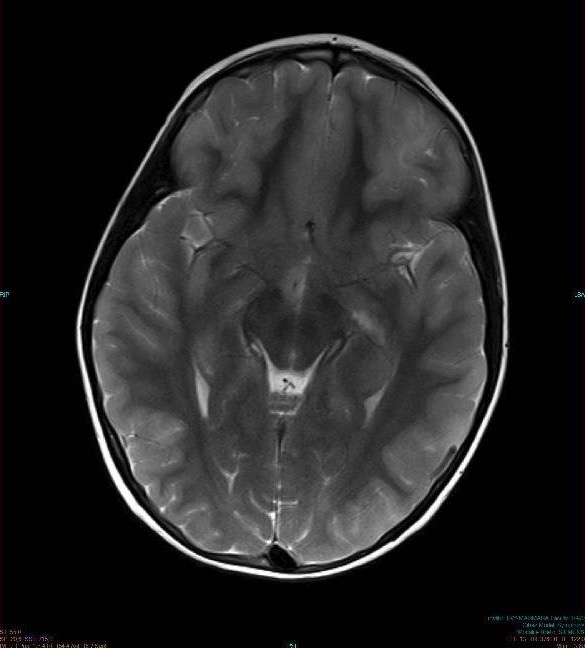
00:00 How do we examine these patients? Well the clinical exam is critical. We're looking for signs of global neurologic dysfunction, we're looking for memory impairment and personality changes, we're assessing vision and frontal function, executive and other frontal functions. 00:15 And ultimately there will be a laboratory evaluation that's common for most infections, a CBC, a complete blood count to look for white blood cells, elevation in white blood cells, or a leukocytosis suggesting infection, the comprehensive metabolic profile will allow us to assess for kidney or liver abnormalities, coagulation tests are done in selected patients particularly prior to a lumbar puncture, and urinalysis can be helpful if we're considering a UTI as a potential bacterial source. Blood in urine cultures are done when we're worried about infections and many institutions and physicians will send a meningoencephalitis panel or a panel to look for all of those potential infections; viral, bacterial, and some other that could be causing this type of presentation. Ultimately, the lumbar puncture is critical and this is how we're going to hone in on infection and understand the type of infection; bacterial, viral, fungal, or parasitic. When we do a cerebrospinal fluid tap, when we look at the CSF, we look at cell count, protein, glucose, and we've seen how those are important. Elevated cell count, pleocytosis with normal to mildly elevated protein and normal glucose is a viral signature. 01:25 Cultures are important on the spinal tap and ultimately if we're looking for viruses, we look for evidence of the virus with viral PCRs and some typical viral PCRs that we would do when we're worried about a viral meningitis or viral encephalitis or viral infection in the brain of any kind would be HSV to look for herpes simplex, VZV to look for varicella zoster, CMV for cytomegalovirus, and Epstein-Barr virus with EBV. Imaging is very important in patients that we're concerned may have an encephalitis and particularly a herpes encephalitis. MRI is extremely sensitive for diagnosing viral encephalitis and what we're looking for is edema in some area of the brain. As we see here on the right, this is a coronal T2 image, and we see increased T2 signal, T2 hyperintensity in the right temporal and insular cortex and maybe extending into the orbitofrontal cortex. Herpes has a predilection, a tropism for the temporal lobes and the orbitofrontal cortex. It likes to go there, it likes to infect those cells. As a result, patients present with memory loss from the hippocampal involvement, personality changes from insular and limbic cortex dysfunction and sometimes frontal dysfunction from prominent orbitofrontal signal abnormalities and infection. But ultimately that virus is affecting all of the brain, all of the subarachnoid space in pia and this results in global neurologic deficit. Imaging is also important because patients may present with a focal onset seizure as was the case for our patient and imaging is important to rule out an abscess which would require different treatment.
About the Lecture
The lecture Encephalitis: Examination by Roy Strowd, MD is from the course CNS Infections.
Included Quiz Questions
Which of the following CSF findings is consistent with viral infection?
- Elevated protein
- Purulent appearance
- Normal cell count
- Decreased glucose
- Decreased opening pressure
What is the imaging modality of choice for diagnosing viral encephalitis?
- Magnetic resonance imaging (MRI)
- Computed tomography (CT) scan
- Ultrasonography
- Plain skull X-ray
- Cerebral angiography
Author of lecture Encephalitis: Examination

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
